


Cristina Quinteiro, Nurse, Santa Casa da Misericórdia Health Unit of Montemor-o-Velho, Portugal
Results and discussion
While several commonly used regimens were ineffective for weeks, a clear wound progression was observed after the first days of L-Mesitran treatment. Although previous treatments were suboptimal, this is often a problem when patients are treated by clinicians lacking current wound care knowledge, or are cared for by family and friends. It is advisable to seek specialist input in any case where a wound has failed to progress two weeks post injury. This particularly applies to patients with known barriers to healing, such as co-morbidities and advanced age, as described in this case. Treatment often focuses on antiseptic properties to clean the wound; however, these products typically do not promote healing. Examples of such antimicrobial treatments include povidone iodine, antibiotics, and silver dressings. Other treatments only keep wounds moist and do not have antimicrobial activity, such as Vaseline and Bepanthen, as used in this case. However, this is not considered best practice and monotherapy with a product such as MGH that cleans the wound while stimulating healing is preferable.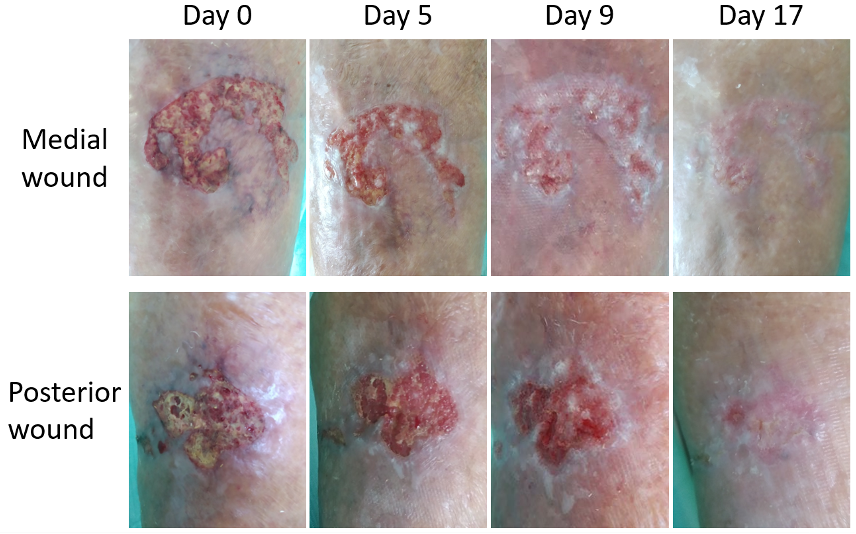
Figure 1. The wound healing progression in time during L-Mesitran treatment
References
Bonifant H, Holloway S (2019) A review of the effects of ageing on skin integrity and wound healing. Br J Community Nurs 24(Sup3): S28–S33
Combarros-Fuertes P, Fresno JM, Estevinho MM, Sousa-Pimenta M, Tornadijo ME, Estevinho LM (2020) Honey: another alternative in the fight against antibiotic-resistant bacteria? Antibiotics (Basel) 9(11): 774; doi: 10.3390/antibiotics9110774
Cremers N, Belas A, Santos Costa S, Couto I, de Rooster H, Pomba C (2020) In vitro antimicrobial efficacy of two medical grade honey formulations against common high-risk meticillin-resistant staphylococci and Pseudomonas spp. pathogens. Vet Dermatol 31(2): 90–96
Gosain A, DiPietro LA (2004) Aging and wound healing. World J Surg 28(3): 321–6
Hermanns R, Mateescu C, Thrasyvoulou A, Tananaki C, Wagener FADTG, Cremers NAJ (2020) Defining the standards for medical grade honey. Journal of Apicultural Research 2020; 59(2): 125–35
Leung E, Wongrakpanich S, Munshi MN (2018) Diabetes Management in the Elderly. Diabetes Spectr 31(3): 245–53
Mandal MD, Mandal S (2011) Honey: its medicinal property and antibacterial activity. Asian Pac J Trop Biomed 1(2): 154–60
Molan PC (2002) Re-introducing honey in the management of wounds and ulcers - theory and practice. Ostomy Wound Manage 48(11): 28–40
Nair HKR, Tatavilis N, Pospisilova I, Kucerova J, Cremers NAJ (2020) Medical-grade honey kills antibiotic-resistant bacteria and prevents amputation in diabetics with infected ulcers: a prospective case series. Antibiotics (Basel) 9(9): 529
Pleeging CCF, Coenye T, Mossialos D, et al (2020) Synergistic antimicrobial activity of supplemented medical-grade honey against Pseudomonas aeruginosa biofilm formation and eradication. Antibiotics 9(12): 866
Renáta Zeleníkováa, Dana Vyhlídalováb (2019) Applying honey dressings to non-healing wounds in elderly persons receiving home care. J Tissue Viability; doi: 10.1016/j.jtv.2019.04.002
Sen CK (2019) Human Wounds and Its Burden: An Updated Compendium of Estimates. Adv Wound Care (New Rochelle. 8(2): 39–48
Smaropoulos E, Cremers NAJ (2019) The pro-healing effects of medical grade honey supported by a pediatric case series. Complement Ther Med 45: 14–18
Smaropoulos E, Cremers NAJ (2020a) Treating severe wounds in pediatrics with medical grade honey: A case series. Clin Case Rep. 8(3): 469–76
Smaropoulos E, Cremers NA (2020b) Medical grade honey for the treatment of paediatric abdominal wounds: a case series. J Wound Care 29(2): 94–9
Smaropoulos E, Cremers NAJ (2021) Medical grade honey for the treatment of extravasation-induced injuries in preterm neonates – a case series. Advances in Neonatal Care 21(2): 122–32
Stechmiller JK (2010) Understanding the role of nutrition and wound healing. Nutr Clin Pract 25(1): 61–8
Wilkinson HN, Hardman MJ (2020) Wound healing: cellular mechanisms and pathological outcomes. Open Biol 10(9): 200223
Yilmaz AC, Aygin D (2020) Honey Dressing in Wound Treatment: A Systematic Review. Complement Ther Med 51: 102388
Zeleníkováa R, Vyhlídalováb D (2019) Applying honey dressings to non-healing wounds in elderly persons receiving home care. J Tissue Viability; doi: 10.1016/j.jtv.2019.04.002
Combarros-Fuertes P, Fresno JM, Estevinho MM, Sousa-Pimenta M, Tornadijo ME, Estevinho LM (2020) Honey: another alternative in the fight against antibiotic-resistant bacteria? Antibiotics (Basel) 9(11): 774; doi: 10.3390/antibiotics9110774
Cremers N, Belas A, Santos Costa S, Couto I, de Rooster H, Pomba C (2020) In vitro antimicrobial efficacy of two medical grade honey formulations against common high-risk meticillin-resistant staphylococci and Pseudomonas spp. pathogens. Vet Dermatol 31(2): 90–96
Gosain A, DiPietro LA (2004) Aging and wound healing. World J Surg 28(3): 321–6
Hermanns R, Mateescu C, Thrasyvoulou A, Tananaki C, Wagener FADTG, Cremers NAJ (2020) Defining the standards for medical grade honey. Journal of Apicultural Research 2020; 59(2): 125–35
Leung E, Wongrakpanich S, Munshi MN (2018) Diabetes Management in the Elderly. Diabetes Spectr 31(3): 245–53
Mandal MD, Mandal S (2011) Honey: its medicinal property and antibacterial activity. Asian Pac J Trop Biomed 1(2): 154–60
Molan PC (2002) Re-introducing honey in the management of wounds and ulcers - theory and practice. Ostomy Wound Manage 48(11): 28–40
Nair HKR, Tatavilis N, Pospisilova I, Kucerova J, Cremers NAJ (2020) Medical-grade honey kills antibiotic-resistant bacteria and prevents amputation in diabetics with infected ulcers: a prospective case series. Antibiotics (Basel) 9(9): 529
Pleeging CCF, Coenye T, Mossialos D, et al (2020) Synergistic antimicrobial activity of supplemented medical-grade honey against Pseudomonas aeruginosa biofilm formation and eradication. Antibiotics 9(12): 866
Renáta Zeleníkováa, Dana Vyhlídalováb (2019) Applying honey dressings to non-healing wounds in elderly persons receiving home care. J Tissue Viability; doi: 10.1016/j.jtv.2019.04.002
Sen CK (2019) Human Wounds and Its Burden: An Updated Compendium of Estimates. Adv Wound Care (New Rochelle. 8(2): 39–48
Smaropoulos E, Cremers NAJ (2019) The pro-healing effects of medical grade honey supported by a pediatric case series. Complement Ther Med 45: 14–18
Smaropoulos E, Cremers NAJ (2020a) Treating severe wounds in pediatrics with medical grade honey: A case series. Clin Case Rep. 8(3): 469–76
Smaropoulos E, Cremers NA (2020b) Medical grade honey for the treatment of paediatric abdominal wounds: a case series. J Wound Care 29(2): 94–9
Smaropoulos E, Cremers NAJ (2021) Medical grade honey for the treatment of extravasation-induced injuries in preterm neonates – a case series. Advances in Neonatal Care 21(2): 122–32
Stechmiller JK (2010) Understanding the role of nutrition and wound healing. Nutr Clin Pract 25(1): 61–8
Wilkinson HN, Hardman MJ (2020) Wound healing: cellular mechanisms and pathological outcomes. Open Biol 10(9): 200223
Yilmaz AC, Aygin D (2020) Honey Dressing in Wound Treatment: A Systematic Review. Complement Ther Med 51: 102388
Zeleníkováa R, Vyhlídalováb D (2019) Applying honey dressings to non-healing wounds in elderly persons receiving home care. J Tissue Viability; doi: 10.1016/j.jtv.2019.04.002