

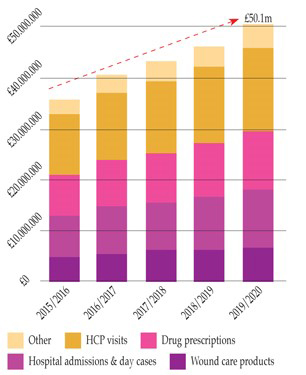
Figure 1. Breakdown in spend and predicted growth of wound care costs at 11% year on year (Guest et al, 2017).
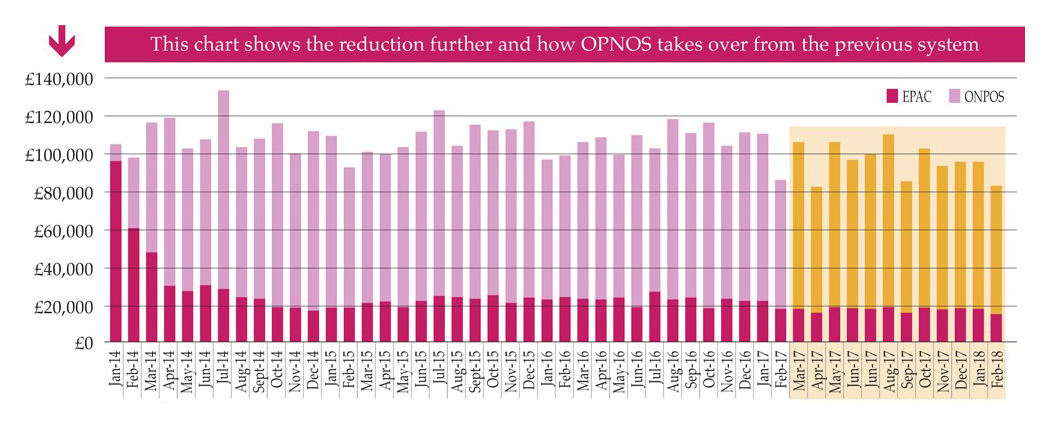
Figure 2. Year on year savings gained by use of ONPOS compared to previously used system
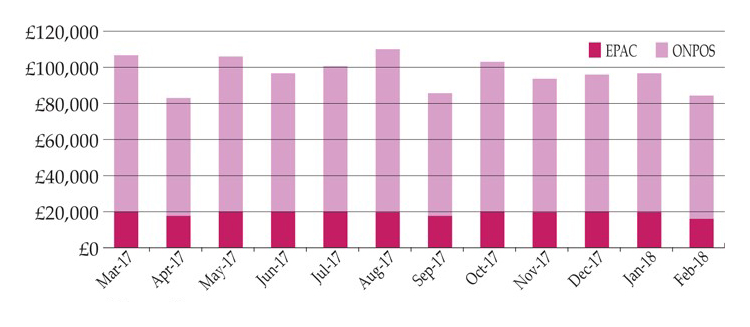
Figure 3. Savings gained by use of ONPOS compared to previously used system
References
Alderwick H, Robertson R, Appleby J, et al (2015) Better value in the NHS: the role of changes in clinical practice. The King’s Fund, London
Barrett S, Markey P (2017) The benefit of using an online ordering service to improve efficiency in wound care services. Br J Health Care Management 23(11): 517–23
Dimond B (2011) Legal Aspects of Nursing. Pearson Education, Harlow
Gray TA, Rhodes S, Atkinson RA, et al (2018) Opportunities for better value wound care: a multiservice, cross-sectional survey of complex wounds and their care in the UK community population. Br Med J Open Access
Griffin J (2015) Driving efficiencies in wound care expenditure through service redesign utilizing an online non-prescription ordering service. Wounds UK 11(3): 1–6
Griffin J (2013) Reviewing the impact of online non-prescription supply of wound care dressings — ONPOS. Poster presentation, Wounds UK, Harrogate
Grothier L (2011) Using ONPOS to implement the QIPP Agenda. Poster presentation, Wound UK, Harrogate
Grothier L (2013) Reflections on the implementation of a web-based non-prescription ordering system. Wounds UK 9(2): 51–5
Guest JF, Ayoub N, McIlwraith T, et al (2015) Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5: e009283. doi:10.1136/bmjopen-2015-009283. Available online: http://bmjopen.bmj.com/content/5/12/e009283
Guest JF, Vowden K, Vowden P (2017) The health economic burden that acute and chronic wounds impose on an average clinical commissioning group/health board in the UK. J Wound Care 26(6): 292–303
Humber NHS Foundation Trust (2013) NOE CPC Case Study. Wound Care dressings community distribution service. North of England NHS Commercial Procurement Collaborative, Humber NHS Foundation Trust
Imbirski K (2013) Utilising ONPOS to change practice and reduce waste within an integrated care team. Poster presentation, Wounds UK, Harrogate
Knight S (2010) Introducing a new method of providing wound care products. Wounds UK 6(2): 66–73
Markey P, Barrett S (2017) The benefits of using an online ordering service to improve efficiency in wound care services. Br J Healthcare Manage 23(11): 1–7
Milne J (2018) Comparison of survey results prior to and 6 months following the introduction of an online non-prescription ordering service. Poster. Wound Care Today, Milton Keynes, June 2018
NHS England (2014) Five Year Forward View. NHS England, London. Available online: www.england.nhs.uk/wp- content/uploads/2014/10/5yfv-web.pdf
North of England NHS Commercial Procurement Collaborative (2013) Wound care dressings community distribution service. North of England NHS Commercial Procurement Collaborative, Humber NHS Foundation Trust
National Prescription Centre (2012) Key Therapeutics Topics – Medicines Management Options for Local Implementation. NICE, London
Porter ME (2010) What is value in health care? N Engl J Med 363: 2477–81
Royal College of Nursing (2013) Frontline First: Nursing on Red Alert April 2013. RCN. London. Available online: https://my.rcn.org.uk/__data/assets/pdf_file/0003/518376/004446.pdf
(accessed 19/09/2017)
Ubbink DT, Santema TB, Stoekenbroek RM (2014) Systemic wound care: a meta-review of Cochrane systematic reviews. Surg Technol Int 24: 99–111
Barrett S, Markey P (2017) The benefit of using an online ordering service to improve efficiency in wound care services. Br J Health Care Management 23(11): 517–23
Dimond B (2011) Legal Aspects of Nursing. Pearson Education, Harlow
Gray TA, Rhodes S, Atkinson RA, et al (2018) Opportunities for better value wound care: a multiservice, cross-sectional survey of complex wounds and their care in the UK community population. Br Med J Open Access
Griffin J (2015) Driving efficiencies in wound care expenditure through service redesign utilizing an online non-prescription ordering service. Wounds UK 11(3): 1–6
Griffin J (2013) Reviewing the impact of online non-prescription supply of wound care dressings — ONPOS. Poster presentation, Wounds UK, Harrogate
Grothier L (2011) Using ONPOS to implement the QIPP Agenda. Poster presentation, Wound UK, Harrogate
Grothier L (2013) Reflections on the implementation of a web-based non-prescription ordering system. Wounds UK 9(2): 51–5
Guest JF, Ayoub N, McIlwraith T, et al (2015) Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5: e009283. doi:10.1136/bmjopen-2015-009283. Available online: http://bmjopen.bmj.com/content/5/12/e009283
Guest JF, Vowden K, Vowden P (2017) The health economic burden that acute and chronic wounds impose on an average clinical commissioning group/health board in the UK. J Wound Care 26(6): 292–303
Humber NHS Foundation Trust (2013) NOE CPC Case Study. Wound Care dressings community distribution service. North of England NHS Commercial Procurement Collaborative, Humber NHS Foundation Trust
Imbirski K (2013) Utilising ONPOS to change practice and reduce waste within an integrated care team. Poster presentation, Wounds UK, Harrogate
Knight S (2010) Introducing a new method of providing wound care products. Wounds UK 6(2): 66–73
Markey P, Barrett S (2017) The benefits of using an online ordering service to improve efficiency in wound care services. Br J Healthcare Manage 23(11): 1–7
Milne J (2018) Comparison of survey results prior to and 6 months following the introduction of an online non-prescription ordering service. Poster. Wound Care Today, Milton Keynes, June 2018
NHS England (2014) Five Year Forward View. NHS England, London. Available online: www.england.nhs.uk/wp- content/uploads/2014/10/5yfv-web.pdf
North of England NHS Commercial Procurement Collaborative (2013) Wound care dressings community distribution service. North of England NHS Commercial Procurement Collaborative, Humber NHS Foundation Trust
National Prescription Centre (2012) Key Therapeutics Topics – Medicines Management Options for Local Implementation. NICE, London
Porter ME (2010) What is value in health care? N Engl J Med 363: 2477–81
Royal College of Nursing (2013) Frontline First: Nursing on Red Alert April 2013. RCN. London. Available online: https://my.rcn.org.uk/__data/assets/pdf_file/0003/518376/004446.pdf
(accessed 19/09/2017)
Ubbink DT, Santema TB, Stoekenbroek RM (2014) Systemic wound care: a meta-review of Cochrane systematic reviews. Surg Technol Int 24: 99–111