


Febe Bruwer, Clinical Nurse Specialist in Wound Care, Woundclinic, Nianwi Healthcare, Johannesburg,
And Vice President of the Wound Healing Association of Southern Africa
A). 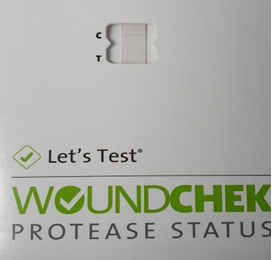
B). 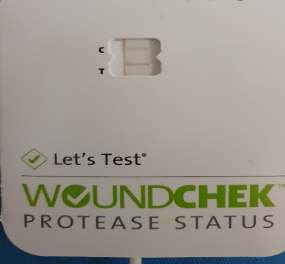
Case 1
A 47-year-old female presented with a traumatic injury to the shin that developed into a chronic ulcer (Figure 2a). The wound was present for about 6 weeks before starting treatment with L-Mesitran. Previous treatment included the topical application of antibiotics. After 25 days of MGH treatment (Figure 2b), protease activity was decreased.
Figure 2. a. The wound on Day 0 of MGH treatment; b. Day 25 of MGH treatment.
Case 2
A 79-year-old female with venous disease presented with a recurrent ulcer (CEAP C6 classification) (Figure 3a). The wound was present for about 6 weeks before L-mesitran treatment, and had previously treated with a topical antibiotic. After one treatment with MGH, the inflammation subsided (Figure 3b) and wound protease levels decreased.Treatment with topical antibiotics, although not advisable, is still a standard treatment in South Africa as the patient’s first contact after injury is the general practitioner or pharmacy. Within the wound care fraternity, topical antibiotic treatment is not the standard of care, but the patients are usually referred to the clinic only after seeing the general practitioner/pharmacy.
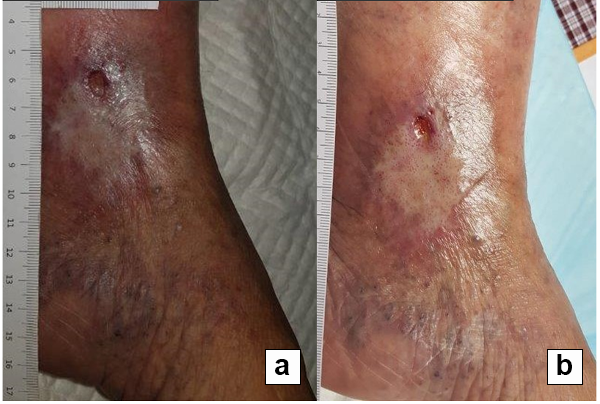
Figure 3. a. The wound on Day 0 of MGH treatment; b. Day 2 of MGH treatment.
Case 3
A 50-year-old male presented with a recurrent venous lower leg ulcer (CEAP C6 classification) (Figure 4a). The wound was present for about 6 months prior to L-Mesitran treatment and was previously treated with paraffin gauze. After 3 weeks L-Mesitran treatment, the wound showed improvement (Figure 4b) and the protease levels were decreased. At our facility compression therapy for the treatment of venous lower leg ulcers is standard care.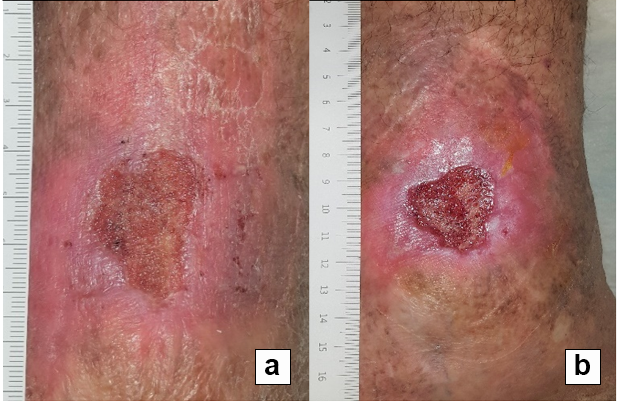
Figure 4. a. The wound on Day 0 of MGH treatment; b. Day 21 of MGH treatment.
Case 4
A 96-year-old male presented with a chronic venous ulcer to the lower leg (Figure 5a). The wound was present for about 6 months and was previously treated with parrafin gauze before starting L-Mesitran treatment. After 45 days, the wound tissue was debrided, more vital and became smaller by reepithelialisation (Figure 5b), and protease activity decreased.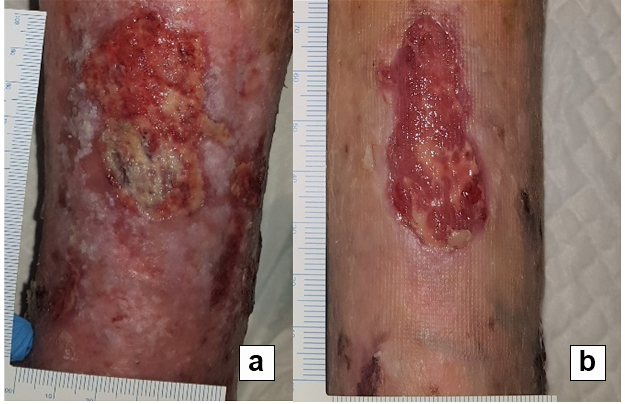
Figure 5. a. The wound on Day 0 of MGH treatment; b. Day 45 of MGH treatment.
Case 5
A 70-year-old male presented with a recurrent ulceration (CEAP C6 classification) (Figure 6a) which was present for about 4 months and previously treated with topical antibiotics. After 6 days, the inflammation subsided, the wound epithelialized and protease activity decreased (Figure 6b).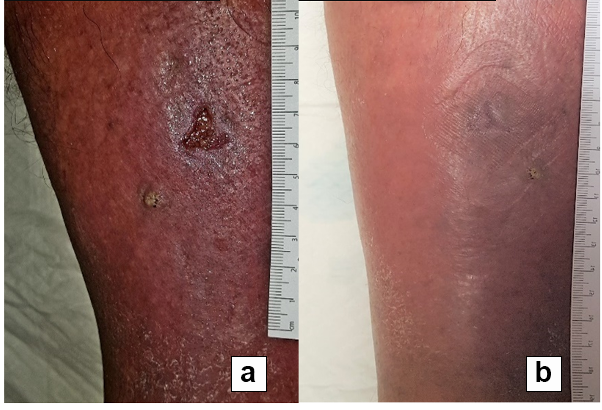
Figure 6. a. The wound on Day 0 of MGH treatment; b. Day 6 of MGH treatment.
Case 6
A 58-year-old male with diabetes had a chronic ulcer on the achilles due to surgery (Figure 7a). The wound was present for 8 months and previously treated with polyurethane foam before starting L-Mesitran treatment. L-Mesitran was applied every second day, until the patient unfortunately discontinued care himself after 14 days. At this timepoint, reepithelialisation was ongoing (Figure 7b) and protease levels were decreased.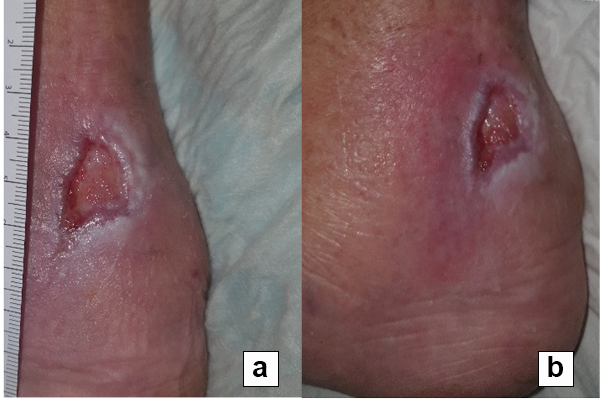
Figure 7. a. The wound on Day 0 of MGH treatment; b. Day 14 of MGH treatment.
Case 7
A 66-year-old male with chronic venous insufficiency had a venous ulcer (CEAP C6 classification) on the lower leg present for more than 2 years (Figure 8a). At day 28, the wound was debrided, granulating, more vital and became smaller by reepithelialisation (Figure 8b), while protease activity was decreased.
Figure 8. a. The wound on Day 0 of MGH treatment; b. Day 28 of MGH treatment.
References
Atkin L (2014) Understanding methods of wound debridement. Br J Nurs 23(12): S10–12, S14–15
Cremers N, Belas A, Santos Costa S, Couto I, de Rooster H, Pomba C (2020) In vitro antimicrobial efficacy of two medical grade honey formulations against common high-risk meticillin-resistant staphylococci and Pseudomonas spp. pathogens. Vet Dermatol 31(2): 90–96
Diegelmann RF, Evans MC (2004) Wound healing: an overview of acute, fibrotic and delayed healing. Front Biosci 9: 283–9
Erfurt-Berge C, Renner R (2014) Recent developments in topical wound therapy: impact of antimicrobiological changes and rebalancing the wound milieu. Biomed Res Int 2014; ID: 819525
Eming SA, Martin P, Tomic-Canic M (2014) Wound repair and regeneration: mechanisms, signaling, and translation. Sci Transl Med 6(265): 265sr6
Gulati S, Qureshi A, Srivastava A, Kataria K, Kumar P, Ji AB (2014) A Prospective Randomized Study to Compare the Effectiveness of Honey Dressing vs. Povidone Iodine Dressing in Chronic Wound Healing. Indian J Surg 76(3):193–8
Hermanns R, Mateescu C, Thrasyvoulou A, Tananaki C, Wagener FADTG, Cremers NAJ (2020) Defining the standards for medical grade honey. Journal of Apicultural Research 59(2): 125–35
International consensus (2011) The role of proteases in wound diagnosis. An Expert working group review. Wounds International 1–13
Martinotti S, Bucekova M, Majtan J, Ranzato E (2018) Honey: an effective regenerative medicine product in wound management. Curr Med Chem 26(27): 5230–40
McCarty SM, Percival SL (2013) Proteases and Delayed Wound Healing. Adv Wound Care (New Rochelle) 2(8): 438–47
Molan P, Rhodes T (2015)Honey: A Biologic Wound Dressing. Wounds 27(6): 141–51 Rundhaug JE (2005) Matrix metalloproteinases and angiogenesis. J Cell Mol Med 9(2): 267–85
Simon A, Traynor K, Santos K, Blaser G, Bode U, Molan P (2009) Medical honey for wound care-still the 'latest resort'? Evid Based Complement Alternat Med 6(2): 165–73
Smaropoulos E, Cremers NA (2020a) Treating severe wounds in pediatrics with medical grade honey: A case series. Clinical Case Reports. 8(3): 469–76
Smaropoulos E, Cremers NA (2020b) Medical grade honey for the treatment of paediatric abdominal wounds: a case series. J Wound Care 29(2): 94–9
Smaropoulos E, Cremers NA (2021) Medical-Grade Honey for the Treatment of Extravasation-Induced Injuries in Preterm Neonates: A Case Series. Adv Neonatal Care 21(2):122-132. DOI: 10.1097/ANC.0000000000000781
Smeets R, Ulrich D, Unglaub F, Woltje M, Pallua N (2008) Effect of oxidised regenerated cellulose/collagen matrix on proteases in wound exudate of patients with chronic venous ulceration. Int Wound J 5(2): 195–203
Westby MJ, Norman G, Dumville JC, Stubbs N, Cullum N (2016) Protease-modulating matrix treatments for healing venous leg ulcers. Cochrane Database Syst Rev. 12: CD011918
Wild T, Rahbarnia A, Kellner M, Sobotka L, Eberlein T (2010) Basics in nutrition and wound healing. Nutrition 26(9): 862–6
Yaghoobi R, Kazerouni A, Kazerouni O (2013) Evidence for Clinical Use of Honey in Wound Healing as an Anti-bacterial, Anti-inflammatory Anti-oxidant and Anti-viral Agent: A Review. Jundishapur J Nat Pharm Prod 8(3): 100–104
Yilmaz AC, Aygin D (2020) Honey Dressing in Wound Treatment: A Systematic Review. Complement Ther Med 51: 102388; doi: 10.1016/j.ctim.2020.102388
Cremers N, Belas A, Santos Costa S, Couto I, de Rooster H, Pomba C (2020) In vitro antimicrobial efficacy of two medical grade honey formulations against common high-risk meticillin-resistant staphylococci and Pseudomonas spp. pathogens. Vet Dermatol 31(2): 90–96
Diegelmann RF, Evans MC (2004) Wound healing: an overview of acute, fibrotic and delayed healing. Front Biosci 9: 283–9
Erfurt-Berge C, Renner R (2014) Recent developments in topical wound therapy: impact of antimicrobiological changes and rebalancing the wound milieu. Biomed Res Int 2014; ID: 819525
Eming SA, Martin P, Tomic-Canic M (2014) Wound repair and regeneration: mechanisms, signaling, and translation. Sci Transl Med 6(265): 265sr6
Gulati S, Qureshi A, Srivastava A, Kataria K, Kumar P, Ji AB (2014) A Prospective Randomized Study to Compare the Effectiveness of Honey Dressing vs. Povidone Iodine Dressing in Chronic Wound Healing. Indian J Surg 76(3):193–8
Hermanns R, Mateescu C, Thrasyvoulou A, Tananaki C, Wagener FADTG, Cremers NAJ (2020) Defining the standards for medical grade honey. Journal of Apicultural Research 59(2): 125–35
International consensus (2011) The role of proteases in wound diagnosis. An Expert working group review. Wounds International 1–13
Martinotti S, Bucekova M, Majtan J, Ranzato E (2018) Honey: an effective regenerative medicine product in wound management. Curr Med Chem 26(27): 5230–40
McCarty SM, Percival SL (2013) Proteases and Delayed Wound Healing. Adv Wound Care (New Rochelle) 2(8): 438–47
Molan P, Rhodes T (2015)Honey: A Biologic Wound Dressing. Wounds 27(6): 141–51 Rundhaug JE (2005) Matrix metalloproteinases and angiogenesis. J Cell Mol Med 9(2): 267–85
Simon A, Traynor K, Santos K, Blaser G, Bode U, Molan P (2009) Medical honey for wound care-still the 'latest resort'? Evid Based Complement Alternat Med 6(2): 165–73
Smaropoulos E, Cremers NA (2020a) Treating severe wounds in pediatrics with medical grade honey: A case series. Clinical Case Reports. 8(3): 469–76
Smaropoulos E, Cremers NA (2020b) Medical grade honey for the treatment of paediatric abdominal wounds: a case series. J Wound Care 29(2): 94–9
Smaropoulos E, Cremers NA (2021) Medical-Grade Honey for the Treatment of Extravasation-Induced Injuries in Preterm Neonates: A Case Series. Adv Neonatal Care 21(2):122-132. DOI: 10.1097/ANC.0000000000000781
Smeets R, Ulrich D, Unglaub F, Woltje M, Pallua N (2008) Effect of oxidised regenerated cellulose/collagen matrix on proteases in wound exudate of patients with chronic venous ulceration. Int Wound J 5(2): 195–203
Westby MJ, Norman G, Dumville JC, Stubbs N, Cullum N (2016) Protease-modulating matrix treatments for healing venous leg ulcers. Cochrane Database Syst Rev. 12: CD011918
Wild T, Rahbarnia A, Kellner M, Sobotka L, Eberlein T (2010) Basics in nutrition and wound healing. Nutrition 26(9): 862–6
Yaghoobi R, Kazerouni A, Kazerouni O (2013) Evidence for Clinical Use of Honey in Wound Healing as an Anti-bacterial, Anti-inflammatory Anti-oxidant and Anti-viral Agent: A Review. Jundishapur J Nat Pharm Prod 8(3): 100–104
Yilmaz AC, Aygin D (2020) Honey Dressing in Wound Treatment: A Systematic Review. Complement Ther Med 51: 102388; doi: 10.1016/j.ctim.2020.102388