



Figure 1a and 1b.


Figure 4.




.png)


Kinesio tape
Kinesio tape is a therapeutic taping technique to alleviate pain and facilitate lymphatic drainage by microscopically lifting the skin (Blanco and Gonzalez, 2020). This lifting effect forms convolutions in the skin, increasing interstitial space and decreasing inflammation in affected areas by allowing blood and lymph to dilate and drain. The tape increases the space in which lymphatic fluid flows, enabling it to move towards working lymph nodes. It can also help to facilitate the stretch response of the angions, with movement or muscle contraction (Blanco and Gonzalez, 2020).Kinesio tape is applied with differing tensions to areas of oedema and fibrosis, following the identified lymphatic drainage pathways identified by the pinch skin test (Figure 8).
Case studies for kinesio tape
Patient F had a haematoma and was also morbidly obese and refused any form of compression. Kinesio taping was started following the lymphatic drainage pathways and the wound healed within three months (Figures 12–12b).
Patient D had lymphovenous disease with lymphorrhea and recurrent fungal infections to the toes, which had not been controlled with conventional toe and stump bandaging techniques and appropriate antifungal treatments (Figure 13). Kinesio tape was applied following the drainage pathways, (Figure 13a) and then a short-stretch 8cm bandage was applied in a figure-of-eight to the ankle and a 10cm bandage applied in a figure-of-eight to below the knee, finishing with 10cm spiral toe-to-knee bandaging. This treatment regimen resulted in the lymphorrhea and superficial ulcer healing within
four weeks.
Patient G had a small retromalleolar ulcer which had not been responding to conventional bandaging techniques or strapping. Kinesio tape was applied over the primary dressing to reduce the fibrosis and assist healing, which subsequently occurred (Figures 14–14b).
Patient H had a venous leg ulcer which had been present for six months with a fibrosed wound bed. A two-layer elastic/inelastic combination bandage system was applied along with kinesio taping to a draining soft spot on the patient’s leg. The periwound fibrosis softened and the wound reduced in size after four weeks of treatment (Figure 15 and 15a).
The patients involved in these case studies were referred to the authors’ specialist wound and lymphoedema service as they were non-healing at six weeks, despite receiving compression therapy. With the introduction of appropriate adjuvant treatment options, the wounds progressed to healing. In the authors’ clinical opinion, the effect of modified therapies on the fibrotic wound bed and periwound skin needs further investigation.

Figure 13

Figure 12.
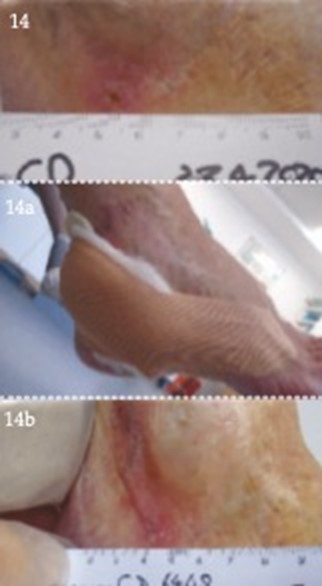
Figure 14

Figure 15
References
Atkin L, Sykes R (2015) Using specialist bandage techniques to improve outcomes. Br J Community Nurs 20(5 Suppl): S8–11
Artlett C M (2012) Inflammasomes in wound healing and fibrosis . J Pathol 229(2): 157–67
Bertelli DF, De Oliver P, Gimenes AS, Morena MA (2013) Postural drainage and manual lymphatic drainage for lower limb oedema in women with morbid obesity after bariatric surgery: a randomised control trial. Am J Phys Med Rehabil 92(8): 697–703
Bjork R (2013) Positive Stemmer’s sign yields a definitive lymphedema diagnosis in 10 seconds or less. Wound Care Advisor 2( 2): 10–14
Bjork R, Hettrick H (2018) Endothelial glycocalyx layer and interdependence of lymphatic and integumentary systems. Wounds Int 9(2): 50–5
Blanco EG, Gonzalez MS (2020) The efficiacy of kinesio taping in the treatment of lymphoedema after breast cancer: a systematic review. J Lymphoedema 15(1): 71–6
Burnand KG, Whimster I, Naidoo A, Browse NL (1982) Pericapillary fibrin in the ulcer-bearing skin of the leg: The cause of lipodermatosclerosis and venous ulceration. Br Med J (Clin Res Ed) 285: 1071–2
Carati CJ, Anderson SN, Gannon BJ, Piller N (2003) Treatment of post mastectomy lymphoedema with low level laser therapy. Cancer 98: 1114–22
Charles H (2103) Chronic oedema, compression therapy and static stiffness index . Wounds UK 9(2) Supplement 2: 4–10
Dyson M, Lyder C (2001) In: Morison MJ, ed. The prevention and treatment of pressure ulcers. Mosby, Edinburgh: 177–93
Ellis M (2015) Lymphovenous disease and its effects on the lower limb. J Community Nurs 29(1): 32–40
Eliska O, Eliskova M (1997) Laser and Lymphatic. Proceedings of 16th ISL congress. Lymphology: 474–7
Elwell R (2015) Compression bandaging for chronic oedema: applying science to reality. Br J Community Nurs 20(5 Suppl): S4–7
European Wound Management Association (2005) Focus Document: Lymphoedema bandage in practice. London: MEP Ltd
Farrow W (2010) Phlebolymphedema – a common underdiagnosed and undertreated problem in the wound care clinic. J Am Col Certif Wound Spec 2(1): 14–23
Finlayson K, Miaskowski C, Alexander K, Lui WH, Aouizerat B, parker C ,Pennis DM , Edwards D (2017) Distinct wound healing and quality of life outcomes in subgroups of patients with venous legs with different cluster experiences. J Pain Symptom Manage 53(5): 871–9
Földi E, Sauerwald A, Hennig B (2000) Effect of complex decongestive physiotherapy on gene expression for the inflammatory response in peripheral lymphedema. Lymphology 33(1): 19–23
Green T (2007) Leg ulcer management in patients with chronic oedema. Wound Essentials 2: 46–58
Guest JF, Ayoub N, McIlwraith T, et al (2015) Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5(12): e009283
Guest JF, Fuller GW, Vowden P (2020) Cohort study evaluating the burden of wounds to the UK’s National Health Service in 2017/2018: update from 2012/2013 BMJ. BMJ Open 10: e045253
Harding K, et al (2015) Simplifying venous leg ulcer management. Consensus recommendations. Wounds International. Available online: www.woundsinternational.com
Hodgson P, Letellier ME, Schumann LH (2011) Use of tissue mobilising compression system. J Lymphoedema 6(2): 91–3
Hopkins A, Worboys F, Bull R, et al (2011) Compression strapping: the development of a novel compression technique to enhance compression therapy and healing for ‘hard-to-heal’ leg ulcers. Inter Wound J 8(5): 474–83
Hopkins A, Worboys F, Partsch H (2013) The use of strapping to increase local pressure: reporting of a sub-bandage pressure study. Veins Lymphatics 2(1): 12
Kozanoglu E, Basaran S, Paydas S, Sarpel T (2009) Efficacy of pneumatic compression and low-level laser therapy in the treatment of postmastectomy lymphoedema: a randomized controlled trial. Clin Rehabil 23(2): 117–24
Macmillan Cancer Suport (2011) Specialist lymphoedema services: An evidence review. Available online: www.Macmillan.org.uk/servicesimpact
Minatel DG, Frade MA, Franca SC, Enwemeka CS (2009) Phototherapy promotes healing of chronic diabetic leg ulcers that failed to respond to other therapies. Lasers Surg Med 41(6): 433–41
Moffatt CJ, Morgan P, Doherty D (2005) The Lymphoedema Framework: a consensus on lymphoedema bandaging. In: European Wound Management Association (EWMA) Focus Document: Lymphoedema bandaging in practice. MEP Ltd, London
Morgan PA, Moody M, Franks PJ, Moffatt CJ, Doherty DC (2005) Assessing community nurses’ level of knowledge of lymphoedema. Br J Nurs 14(1): 8–13
Mortimer P, Browse N (2003) The relationship between the lymphatics and chronic venous disease. In: Browse N, Burnand KG, Mortimer PS (2003) Diseases of the Lymphatics. Arnold, London: 293–6
Mosti G, Cavezzi A, Partsch H, Urso S, Campana F (2015) Adjustable Velcro wrap devices are more effective than inelastic compression bandages in reducing oedema in the initial treatment phase: a randomised control trial. Eur Vas Endovasc Surg 50(3): 368–74
Omar MT, Shaheen AA, Zafar H (2012) A systematic review of the effect of low-level laser therapy in the management of breast cancer-related lymphedema. Support Care Cancer 20(11): 2977–84
Partsch H, Mortimer P (2015) Compression for leg wounds. Br J Dermatol 173(2): 359–69
Piller N, Thelander A (1998) Treating chronic post mastectomy lymphoedema with low level laser therapy: a cost effective strategy to reduce lymphoedema severity and improve the quality of patient life. Lymphology 31(2): 74–86
Schubert V (2001) Effects of phototherapy on pressure ulcer healing in elderly patients after a falling trauma. A prospective, randomized, controlled study. Photodermatol Photoimmunol Photomed 17(1): 32–8
Stanton J (2020) Development of the hybrid tissue viability nurse/lymphoedema nurse. J Community Nurs 34(4): 46–51
Todd M (2019) Chronic oedema: impact and management. Br J Nurs 22(11): 623–7
White R, Price P, Whittaker J, Williams SA (2014) Lymphovenous oedema (phlebolymphoedema): The nature and extent of the problem. Wounds UK 10(1): 22–8
Whittaker J Williams A, Pope D, et al (2015) Clinical audit of a lymphoedema bandaging system: a foam roll and cohesive short stretch bandages. J Wound Care 24(3): 83–4; 86–90; 92–4
Wigg J (2009) Use and response to treatment using low level laser therapy. J Lymphoedema 4(2): 73–6
Wigg J (2015) The Complete Package, Lymphoedema Management (FG-MLD® training), training manual. Lymphoedema Training academy
Wigg J (2016) Fluoroscopy guided manual lymphatic drainage from research to the classroom. International Lymphoedema Framework Conference/Australasian Lymphology Association Conference
Williams A (2003) An overview of non-cancer related chronic oedema — a UK perspective. Worldwide Wounds. Available online: www.worldwidewounds.com/2003/april/Williams/Chronic-Oedema.html
Williams A (2009) Chronic oedema in patients with CVI and ulceration of the lower limb. Br J Community Nurs 14(10): S4–8
Wound Care People (2019) Best practice in the community. Chronic oedema. Wound Care People, Wixford
Wounds UK (2019) Best Practice Statement: Addressing complexities in the management of venous leg ulcers. London: Wounds UK. Available to download from: www.wounds-uk.com
Artlett C M (2012) Inflammasomes in wound healing and fibrosis . J Pathol 229(2): 157–67
Bertelli DF, De Oliver P, Gimenes AS, Morena MA (2013) Postural drainage and manual lymphatic drainage for lower limb oedema in women with morbid obesity after bariatric surgery: a randomised control trial. Am J Phys Med Rehabil 92(8): 697–703
Bjork R (2013) Positive Stemmer’s sign yields a definitive lymphedema diagnosis in 10 seconds or less. Wound Care Advisor 2( 2): 10–14
Bjork R, Hettrick H (2018) Endothelial glycocalyx layer and interdependence of lymphatic and integumentary systems. Wounds Int 9(2): 50–5
Blanco EG, Gonzalez MS (2020) The efficiacy of kinesio taping in the treatment of lymphoedema after breast cancer: a systematic review. J Lymphoedema 15(1): 71–6
Burnand KG, Whimster I, Naidoo A, Browse NL (1982) Pericapillary fibrin in the ulcer-bearing skin of the leg: The cause of lipodermatosclerosis and venous ulceration. Br Med J (Clin Res Ed) 285: 1071–2
Carati CJ, Anderson SN, Gannon BJ, Piller N (2003) Treatment of post mastectomy lymphoedema with low level laser therapy. Cancer 98: 1114–22
Charles H (2103) Chronic oedema, compression therapy and static stiffness index . Wounds UK 9(2) Supplement 2: 4–10
Dyson M, Lyder C (2001) In: Morison MJ, ed. The prevention and treatment of pressure ulcers. Mosby, Edinburgh: 177–93
Ellis M (2015) Lymphovenous disease and its effects on the lower limb. J Community Nurs 29(1): 32–40
Eliska O, Eliskova M (1997) Laser and Lymphatic. Proceedings of 16th ISL congress. Lymphology: 474–7
Elwell R (2015) Compression bandaging for chronic oedema: applying science to reality. Br J Community Nurs 20(5 Suppl): S4–7
European Wound Management Association (2005) Focus Document: Lymphoedema bandage in practice. London: MEP Ltd
Farrow W (2010) Phlebolymphedema – a common underdiagnosed and undertreated problem in the wound care clinic. J Am Col Certif Wound Spec 2(1): 14–23
Finlayson K, Miaskowski C, Alexander K, Lui WH, Aouizerat B, parker C ,Pennis DM , Edwards D (2017) Distinct wound healing and quality of life outcomes in subgroups of patients with venous legs with different cluster experiences. J Pain Symptom Manage 53(5): 871–9
Földi E, Sauerwald A, Hennig B (2000) Effect of complex decongestive physiotherapy on gene expression for the inflammatory response in peripheral lymphedema. Lymphology 33(1): 19–23
Green T (2007) Leg ulcer management in patients with chronic oedema. Wound Essentials 2: 46–58
Guest JF, Ayoub N, McIlwraith T, et al (2015) Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5(12): e009283
Guest JF, Fuller GW, Vowden P (2020) Cohort study evaluating the burden of wounds to the UK’s National Health Service in 2017/2018: update from 2012/2013 BMJ. BMJ Open 10: e045253
Harding K, et al (2015) Simplifying venous leg ulcer management. Consensus recommendations. Wounds International. Available online: www.woundsinternational.com
Hodgson P, Letellier ME, Schumann LH (2011) Use of tissue mobilising compression system. J Lymphoedema 6(2): 91–3
Hopkins A, Worboys F, Bull R, et al (2011) Compression strapping: the development of a novel compression technique to enhance compression therapy and healing for ‘hard-to-heal’ leg ulcers. Inter Wound J 8(5): 474–83
Hopkins A, Worboys F, Partsch H (2013) The use of strapping to increase local pressure: reporting of a sub-bandage pressure study. Veins Lymphatics 2(1): 12
Kozanoglu E, Basaran S, Paydas S, Sarpel T (2009) Efficacy of pneumatic compression and low-level laser therapy in the treatment of postmastectomy lymphoedema: a randomized controlled trial. Clin Rehabil 23(2): 117–24
Macmillan Cancer Suport (2011) Specialist lymphoedema services: An evidence review. Available online: www.Macmillan.org.uk/servicesimpact
Minatel DG, Frade MA, Franca SC, Enwemeka CS (2009) Phototherapy promotes healing of chronic diabetic leg ulcers that failed to respond to other therapies. Lasers Surg Med 41(6): 433–41
Moffatt CJ, Morgan P, Doherty D (2005) The Lymphoedema Framework: a consensus on lymphoedema bandaging. In: European Wound Management Association (EWMA) Focus Document: Lymphoedema bandaging in practice. MEP Ltd, London
Morgan PA, Moody M, Franks PJ, Moffatt CJ, Doherty DC (2005) Assessing community nurses’ level of knowledge of lymphoedema. Br J Nurs 14(1): 8–13
Mortimer P, Browse N (2003) The relationship between the lymphatics and chronic venous disease. In: Browse N, Burnand KG, Mortimer PS (2003) Diseases of the Lymphatics. Arnold, London: 293–6
Mosti G, Cavezzi A, Partsch H, Urso S, Campana F (2015) Adjustable Velcro wrap devices are more effective than inelastic compression bandages in reducing oedema in the initial treatment phase: a randomised control trial. Eur Vas Endovasc Surg 50(3): 368–74
Omar MT, Shaheen AA, Zafar H (2012) A systematic review of the effect of low-level laser therapy in the management of breast cancer-related lymphedema. Support Care Cancer 20(11): 2977–84
Partsch H, Mortimer P (2015) Compression for leg wounds. Br J Dermatol 173(2): 359–69
Piller N, Thelander A (1998) Treating chronic post mastectomy lymphoedema with low level laser therapy: a cost effective strategy to reduce lymphoedema severity and improve the quality of patient life. Lymphology 31(2): 74–86
Schubert V (2001) Effects of phototherapy on pressure ulcer healing in elderly patients after a falling trauma. A prospective, randomized, controlled study. Photodermatol Photoimmunol Photomed 17(1): 32–8
Stanton J (2020) Development of the hybrid tissue viability nurse/lymphoedema nurse. J Community Nurs 34(4): 46–51
Todd M (2019) Chronic oedema: impact and management. Br J Nurs 22(11): 623–7
White R, Price P, Whittaker J, Williams SA (2014) Lymphovenous oedema (phlebolymphoedema): The nature and extent of the problem. Wounds UK 10(1): 22–8
Whittaker J Williams A, Pope D, et al (2015) Clinical audit of a lymphoedema bandaging system: a foam roll and cohesive short stretch bandages. J Wound Care 24(3): 83–4; 86–90; 92–4
Wigg J (2009) Use and response to treatment using low level laser therapy. J Lymphoedema 4(2): 73–6
Wigg J (2015) The Complete Package, Lymphoedema Management (FG-MLD® training), training manual. Lymphoedema Training academy
Wigg J (2016) Fluoroscopy guided manual lymphatic drainage from research to the classroom. International Lymphoedema Framework Conference/Australasian Lymphology Association Conference
Williams A (2003) An overview of non-cancer related chronic oedema — a UK perspective. Worldwide Wounds. Available online: www.worldwidewounds.com/2003/april/Williams/Chronic-Oedema.html
Williams A (2009) Chronic oedema in patients with CVI and ulceration of the lower limb. Br J Community Nurs 14(10): S4–8
Wound Care People (2019) Best practice in the community. Chronic oedema. Wound Care People, Wixford
Wounds UK (2019) Best Practice Statement: Addressing complexities in the management of venous leg ulcers. London: Wounds UK. Available to download from: www.wounds-uk.com