

Silver spend
Inappropriate spend on silver dressings was highlighted by Dowley and Tomes (2018) when ONPOS was implemented in Brighton and Hove NHS Trust. Similarly, the three months of data collected in Royal Wolverhampton highlighted a high spend on silver fillers. When practice was looked at, numerous products were being used as fillers unnecessarily. An education event was subsequently held on the appropriate use of silver dressings and fillers.A pathway for wound infection management was also developed for trust services and formulary products were allocated to stages on the wound infection continuum, to further provide guidance on appropriate silver dressing use (Figure 1).
Following this combined approach, the spend on silver fillers dropped from £8–9K per month to £2–3K per month as a result of education and better product usage. The reduced spend from 17/18 pre-ONPOS to spend post ONPOS use in 2019/20 can be seen in Figure 2.

Figure 2.
Reduced spend on silver fillers for 19/20 (based on first five months of 2019) compared to pre-ONPOS spend.
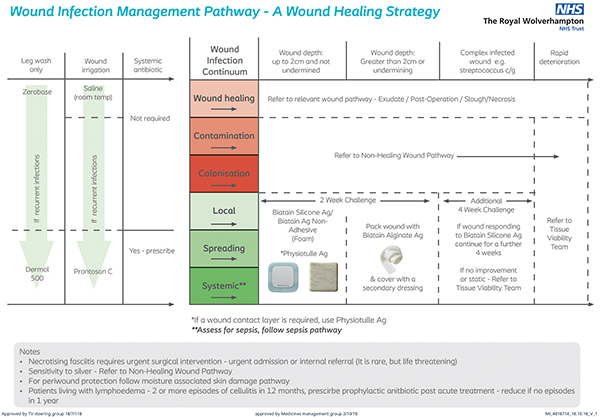
Figure 1.
Wound infection pathway.
Wound infection pathway.

Figure 3. Reduced spend on superabsorbent wound dressings following implementation of ONPOS.
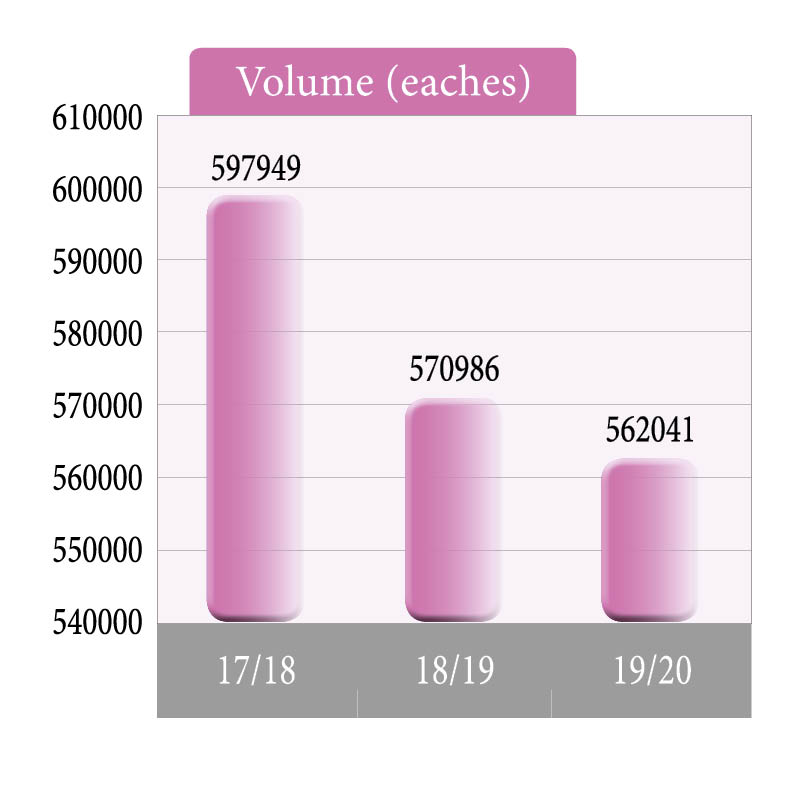
Figure 4. The volume of dressings purchased was reduced following the installation of ONPOS in 2019/20.
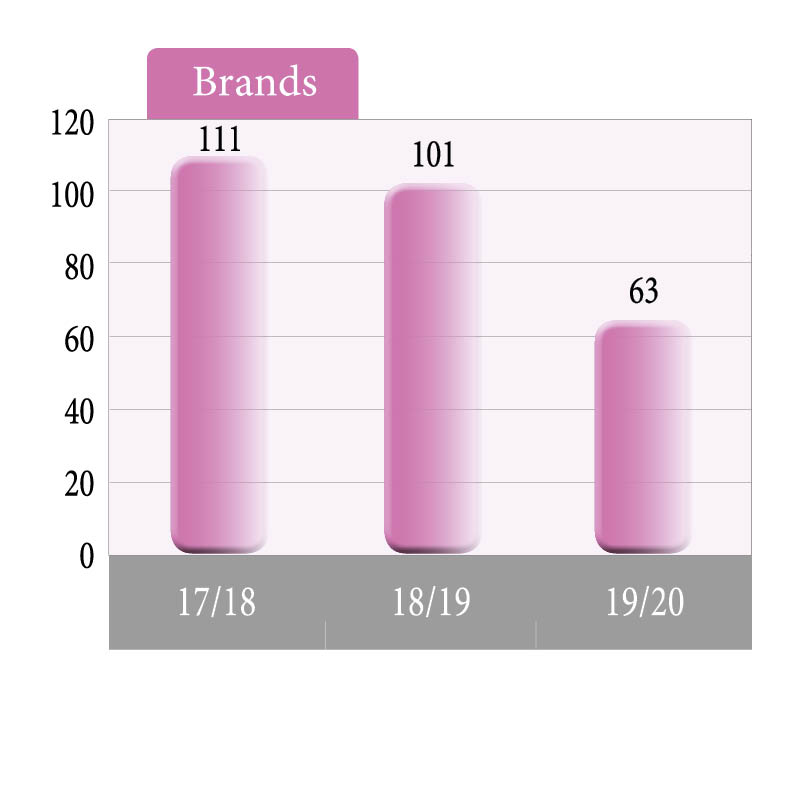
Figure 5. The number of wound care brands included in the wound care formulary was almost halved following the use of ONPOS.
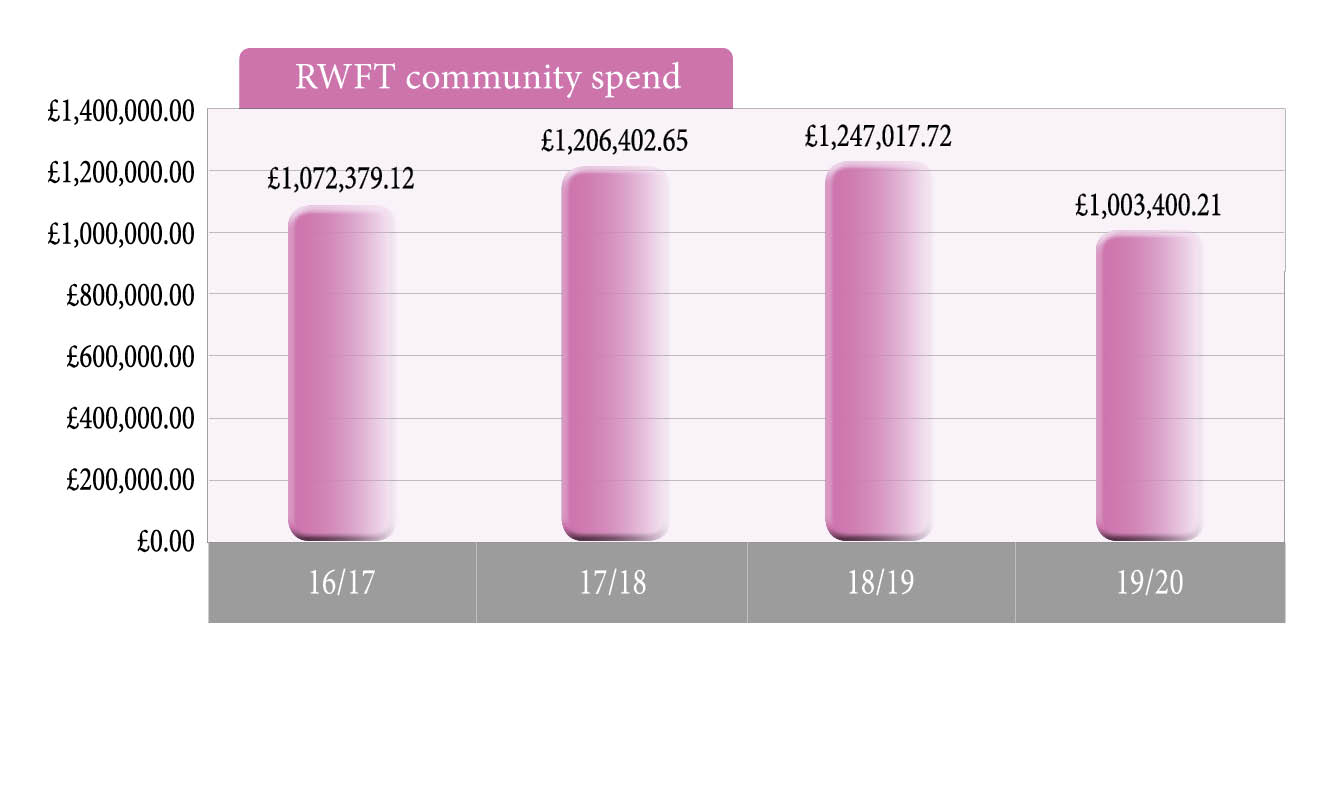
Figure 6. Predicted savings in wound care product spend in the community in 2019/20, following installation of ONPOS.
References
Adderley U (2018) The National Wound Care Strategy Programme. Available online: www.woundcare-today.com/journals/issue/wound-care-today/article/national-wound-care-strategy-programme
Alderwick H, Robertson R, Appleby J, et al (2015) Better value in the NHS: the role of changes in clinical practice. The King’s Fund, London
Department of Health (2012) Report. Long-term conditions compendium of information. Third edn. DH, London
Dowsett C, Bielby A, Searle R (2014) Reconciling increasing wound care demands with available resources. J Wound Care 23(11): 552–62
Dowley V, Tomes J (2018) Implementation and use of ONPOS to drive efficiency and cost-savings in an average-sized CCG. Available online: www.woundcare-today.com/journals/issue/wound-care-today/article/onpos-implementation-drive-efficiency-and-cost-savings
Gray TA, Rhodes S, Atkinson RA, et al (2018) Opportunities for better value wound care: a multiservice, cross-sectional survey of complex wounds and their care in the UK community population. Br Med J Open Access
Griffin J (2013) Reviewing the impact of online non-prescription supply of wound care dressings — ONPOS. Poster presentation, Wounds UK, Harrogate
Griffin J (2015) Driving efficiencies in wound care expenditure through service redesign utilizing an online non-prescription ordering service. Wounds UK 11(3): 1–6
Grothier L (2011) Using ONPOS to implement the QIPP Agenda. Poster presentation, Wound UK, Harrogate
Grothier L (2013) Reflections on the implementation of a web-based non-prescription ordering system. Wounds UK 9(2): 51–5
Guest JF, Ayoub N, McIlwraith T, et al (2015) Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5: e009283. Available online: http://bmjopen.bmj.com/content/5/12/e009283
Guest JF, Vowden K, Vowden P (2017) The health economic burden that acute and chronic wounds impose on an average clinical commissioning group/health board in the UK. J Wound Care 26(6): 292–303
Imbirski K (2013) Utilising ONPOS to change practice and reduce waste within an integrated care team. Poster presentation, Wounds UK, Harrogate
Knight S (2010) Introducing a new method of providing wound care products. Wounds UK 6(2): 66–73
Markey P, Barrett S (2017) The benefits of using an online ordering service to improve efficiency in wound care services. Br J Healthcare Manage
23(11): 1–7
Milne J (2018) Comparison of survey results prior to and 6 months following the introduction of an online non-prescription ordering service. Poster presentation, Wound Care Today, Milton Keynes
National Prescription Centre (2012) Key Therapeutics Topics — Medicines Management Options for Local Implementation. NICE, London
NHS England (2014) Five Year Forward View. NHS England, London. Available online: www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf
NHS England (2018) Leading Change, Adding Value: A framework for nursing, midwifery and care staff. Available online: www.england.nhs.uk/wp-content/uploads/2018/05/lcav-e-learning-tool-v1.pdf
NHS England (2019) NHS Long-term Plan. Available online: www.england.nhs.uk/long-term-plan
Office of National statistics (2017) Available online: www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/articles/overviewoftheukpopulation/july2017
Ubbink DT, Santema TB, Stoekenbroek RM (2014) Systemic wound care: a meta-review of Cochrane systematic reviews. Surg Technol Int 24: 99–111
Alderwick H, Robertson R, Appleby J, et al (2015) Better value in the NHS: the role of changes in clinical practice. The King’s Fund, London
Department of Health (2012) Report. Long-term conditions compendium of information. Third edn. DH, London
Dowsett C, Bielby A, Searle R (2014) Reconciling increasing wound care demands with available resources. J Wound Care 23(11): 552–62
Dowley V, Tomes J (2018) Implementation and use of ONPOS to drive efficiency and cost-savings in an average-sized CCG. Available online: www.woundcare-today.com/journals/issue/wound-care-today/article/onpos-implementation-drive-efficiency-and-cost-savings
Gray TA, Rhodes S, Atkinson RA, et al (2018) Opportunities for better value wound care: a multiservice, cross-sectional survey of complex wounds and their care in the UK community population. Br Med J Open Access
Griffin J (2013) Reviewing the impact of online non-prescription supply of wound care dressings — ONPOS. Poster presentation, Wounds UK, Harrogate
Griffin J (2015) Driving efficiencies in wound care expenditure through service redesign utilizing an online non-prescription ordering service. Wounds UK 11(3): 1–6
Grothier L (2011) Using ONPOS to implement the QIPP Agenda. Poster presentation, Wound UK, Harrogate
Grothier L (2013) Reflections on the implementation of a web-based non-prescription ordering system. Wounds UK 9(2): 51–5
Guest JF, Ayoub N, McIlwraith T, et al (2015) Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5: e009283. Available online: http://bmjopen.bmj.com/content/5/12/e009283
Guest JF, Vowden K, Vowden P (2017) The health economic burden that acute and chronic wounds impose on an average clinical commissioning group/health board in the UK. J Wound Care 26(6): 292–303
Imbirski K (2013) Utilising ONPOS to change practice and reduce waste within an integrated care team. Poster presentation, Wounds UK, Harrogate
Knight S (2010) Introducing a new method of providing wound care products. Wounds UK 6(2): 66–73
Markey P, Barrett S (2017) The benefits of using an online ordering service to improve efficiency in wound care services. Br J Healthcare Manage
23(11): 1–7
Milne J (2018) Comparison of survey results prior to and 6 months following the introduction of an online non-prescription ordering service. Poster presentation, Wound Care Today, Milton Keynes
National Prescription Centre (2012) Key Therapeutics Topics — Medicines Management Options for Local Implementation. NICE, London
NHS England (2014) Five Year Forward View. NHS England, London. Available online: www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf
NHS England (2018) Leading Change, Adding Value: A framework for nursing, midwifery and care staff. Available online: www.england.nhs.uk/wp-content/uploads/2018/05/lcav-e-learning-tool-v1.pdf
NHS England (2019) NHS Long-term Plan. Available online: www.england.nhs.uk/long-term-plan
Office of National statistics (2017) Available online: www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/articles/overviewoftheukpopulation/july2017
Ubbink DT, Santema TB, Stoekenbroek RM (2014) Systemic wound care: a meta-review of Cochrane systematic reviews. Surg Technol Int 24: 99–111