


Figure 1. Venous leg ulcer

Figure 2. Arterial ulcer.

Figure 3. Ulcer due to pyoderma gandrenosum.

Figure 4. Ulcer due to small vessel vasculitis.

Figure 5. Rheumatoid ulcer.

Figure 6. Rheumatoid ulcer.

Figure 7. Ulcer due to calciphylaxis.
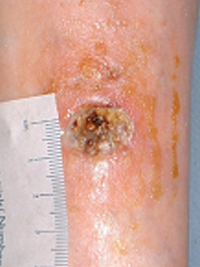
Figure 8. Ulcer due to calcinosis cutis.

Figure 9. Lesion due to basal cell carcinoma.

Figure 10. Ulcer caused by squamous cell carcinoma.
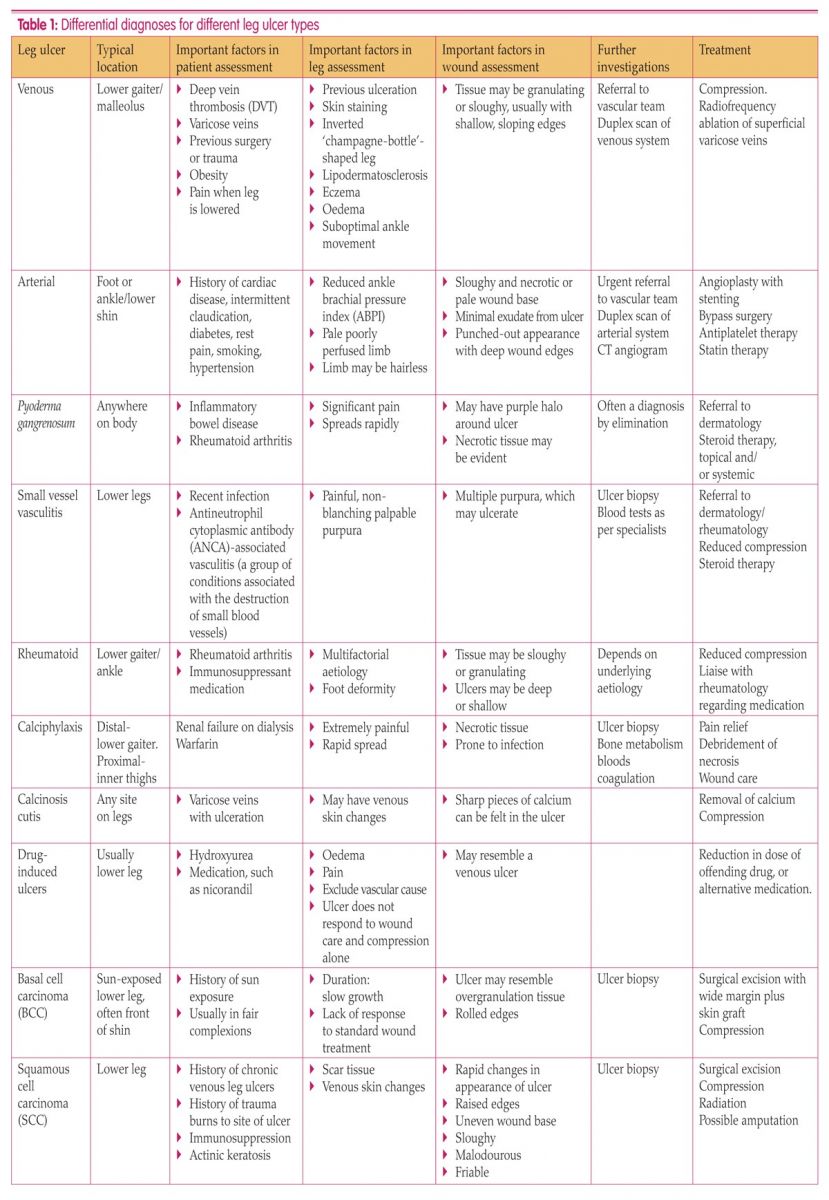
Table 1 summarises the differential diagnoses for a range of leg ulcer types.
References
Anderson I (2006) Aetiology, assessment and management of leg ulcers. Wound Essentials 1: 20–37
Anderson I (2012) Multidimensional leg ulcer assessment. Nurs Times 108(13): 17-20
Anderson (2018) Can this be the moment for leg ulcers? Br J Nurs 27(6): S4
Beldon, P (2011) Ten top tips for doppler ABPI. Wounds Int 2(4): 18–21
Bliss DE (2002) Calciphylaxis: What nurses need to know. Nephrol Nurs J 29(5): 433–8
British Associaton of Dermatology (2017) Cyclosporine. Available online: http://skinsupport.org.uk/conditions-details/ciclosporin (accessed 30 January, 2019)
Burnand KG, Whimster I, Naidoo A, Browse NL. (1982) Pericapillary fibrin in the ulcer-bearing skin of the leg: The cause of lipodermatosclerosis and venous ulceration. Br Med J (Clin Res Ed) 285: 1071–2
Circulation Foundation (2018) Leg ulcers. Available online: www.circulationfoundation.org.uk/help-advice/veins/leg-ulcers (accessed 10 December, 2018)
Etufugh C, Phillips T, Goldberg L, Jensen, S (2005) Squamous cell carcinoma. Wounds 17(11): 321–6
European Wound Management Association (2019) Atypical wounds. Available online: http://ewma.org/what-we-do/ewma-projects-old/we-are-currently-working-on/atypical-wounds/ (accessed 10 January, 2019)
Fletcher J (2007) Wound assessment and the TIME Framework. Br J Nurs 16(8): 462–6
Fukaya E, Margolis DJ (2013) Approach to diagnosing lower extremity ulcers. Dermatol Therap 26: 181–6
Goldie C, Brown J (2012) Managing obesity in primary care. Nurs Times 108(1/2): 14–6
Guest JF, Ayoub N, McIlwraith T, et al (2015) Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5: e009283. doi: 10.1136/bmjopen-2015-009283
Guest JF, Ayoub N, McIlwraith T, et al (2016) Health economic burden that different wound types impose on the UK’s National Health Service. Int Wound J 14(2): 322–30
Harding K, Dowestt C, Fias L, et al (2015) Simplifying enous leg ulcer management. Consensus recommendations. Wounds International. Available online: www.woundsinternational.com (accessed 10 January, 2019)
Huilaja L, Turpeinen M, Tokola H, Kauma H, Tasanen K, Ikaheimo R (2016) Warfarin-induced calciphylaxis in patients with normal renal function. J Clin Pharm Ther 41(4): 449–52
Legs Matter (2018) Available online: https://legsmatter.org (accessed 10 January, 2019)
Matthew Q, Pompeo MD (2016) Pyoderma gangrenosum: recognition and management. Wounds 28(1): 7–13
Meyer V, Kerk N, Meyer S, Goerge T (2011) Differential diagnosis and therapy of leg ulcers. J Ditsch Dermatol Ges 9(12): 1035–51
Motley R, Kersey P, Lawrence C (2003) Multiprofessional guidelines for the management of the patient with primary cutaneous squamous cell carcinoma. Br J Plast Surg 56(2): 85–91
NHS England (2016) Commissioning for quality and innovation (CQUIN) guidance for 2017-2019. Available online: www.england.nhs.uk/wp-content/uploads/2018/04/cquin-guidance-2018-19.pdf
NHS England (2017) NHS RightCare scenario: the variation between sub-optimal and optimal pathways. Betty’s story: leg ulcer wound care. Available online: https://tinyurl.com/ bettysstory (accessed 10 December, 2018)
Oakley A (2016) Differential diagnosis of leg ulcer. Available online: www.dermnetnz.org/topics/differential-diagnosis-of-leg-ulcer/ (accessed 10 December, 2018)
Pieper B, Kirsner RS, Templin TN, et al (2007) Injection drug use. Arch Dermatol 143(10): 1305–09
Rayner R, Carville K, Keaton J, Prentice J, Santamaria N (2009) Leg ulcers: atypical presentations and associated comorbidities. Wound Prac Res 17(4): 168–85
Reich-Schupke S, Doerler M, Wollina U, et al (2015) Squamous cell carcinoma in chronic venous leg ulcers. Data of the German Marjolin Registry and review. J Ditsch Dermatol Ges 13(10): 1006–13
Roewert-Huber J, Lange-Asschenfeldt B, Stockfleth E, Kerl H (2007) Epidemiology and aetiology of basal cell carcinoma. Br J Dermatol 157 Suppl 2: 47–51
Royal College of Nursing (2000) The Management of Patients With Venous Leg Ulcers. RCN, London. Available online: www.rcn.org.uk/professional-development/publications/pub-001269 (accessed January 2019)
Santilli MD, Santilli SM (1999) Chronic critical limb ischaemia: Diagnosis, treatment and prognosis. Am Fam Physician 59(7): 1899–1908. Available online: www.aafp.org/afp/1999/0401/p1899.html (accessed 10 January, 2019)
Telfer NR, Colver GB, Morton CA (2008) Guidelines for the management of basal cell carcinoma. Br J Dermatol 159: 35–48
Tobón J, Whitney JD, Jarrett M (2008) Nutritional status and wound severity of overweight and obese patients with venous leg ulcers: a pilot study. J Vasc Nurs 26(2): 43–52
Tokoro S, Satoh T, Okubo Y, Igawa K and Yokozeki H (2009) Latent dystrophic subcutaneous calcification in patients with chronic venous insufficiency. Acta Derma Venereol 89: 505–8
Wounds UK (2016) Best Practice Statement: Holistic management of venous leg ulceration. Wounds UK, London
Anderson I (2012) Multidimensional leg ulcer assessment. Nurs Times 108(13): 17-20
Anderson (2018) Can this be the moment for leg ulcers? Br J Nurs 27(6): S4
Beldon, P (2011) Ten top tips for doppler ABPI. Wounds Int 2(4): 18–21
Bliss DE (2002) Calciphylaxis: What nurses need to know. Nephrol Nurs J 29(5): 433–8
British Associaton of Dermatology (2017) Cyclosporine. Available online: http://skinsupport.org.uk/conditions-details/ciclosporin (accessed 30 January, 2019)
Burnand KG, Whimster I, Naidoo A, Browse NL. (1982) Pericapillary fibrin in the ulcer-bearing skin of the leg: The cause of lipodermatosclerosis and venous ulceration. Br Med J (Clin Res Ed) 285: 1071–2
Circulation Foundation (2018) Leg ulcers. Available online: www.circulationfoundation.org.uk/help-advice/veins/leg-ulcers (accessed 10 December, 2018)
Etufugh C, Phillips T, Goldberg L, Jensen, S (2005) Squamous cell carcinoma. Wounds 17(11): 321–6
European Wound Management Association (2019) Atypical wounds. Available online: http://ewma.org/what-we-do/ewma-projects-old/we-are-currently-working-on/atypical-wounds/ (accessed 10 January, 2019)
Fletcher J (2007) Wound assessment and the TIME Framework. Br J Nurs 16(8): 462–6
Fukaya E, Margolis DJ (2013) Approach to diagnosing lower extremity ulcers. Dermatol Therap 26: 181–6
Goldie C, Brown J (2012) Managing obesity in primary care. Nurs Times 108(1/2): 14–6
Guest JF, Ayoub N, McIlwraith T, et al (2015) Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5: e009283. doi: 10.1136/bmjopen-2015-009283
Guest JF, Ayoub N, McIlwraith T, et al (2016) Health economic burden that different wound types impose on the UK’s National Health Service. Int Wound J 14(2): 322–30
Harding K, Dowestt C, Fias L, et al (2015) Simplifying enous leg ulcer management. Consensus recommendations. Wounds International. Available online: www.woundsinternational.com (accessed 10 January, 2019)
Huilaja L, Turpeinen M, Tokola H, Kauma H, Tasanen K, Ikaheimo R (2016) Warfarin-induced calciphylaxis in patients with normal renal function. J Clin Pharm Ther 41(4): 449–52
Legs Matter (2018) Available online: https://legsmatter.org (accessed 10 January, 2019)
Matthew Q, Pompeo MD (2016) Pyoderma gangrenosum: recognition and management. Wounds 28(1): 7–13
Meyer V, Kerk N, Meyer S, Goerge T (2011) Differential diagnosis and therapy of leg ulcers. J Ditsch Dermatol Ges 9(12): 1035–51
Motley R, Kersey P, Lawrence C (2003) Multiprofessional guidelines for the management of the patient with primary cutaneous squamous cell carcinoma. Br J Plast Surg 56(2): 85–91
NHS England (2016) Commissioning for quality and innovation (CQUIN) guidance for 2017-2019. Available online: www.england.nhs.uk/wp-content/uploads/2018/04/cquin-guidance-2018-19.pdf
NHS England (2017) NHS RightCare scenario: the variation between sub-optimal and optimal pathways. Betty’s story: leg ulcer wound care. Available online: https://tinyurl.com/ bettysstory (accessed 10 December, 2018)
Oakley A (2016) Differential diagnosis of leg ulcer. Available online: www.dermnetnz.org/topics/differential-diagnosis-of-leg-ulcer/ (accessed 10 December, 2018)
Pieper B, Kirsner RS, Templin TN, et al (2007) Injection drug use. Arch Dermatol 143(10): 1305–09
Rayner R, Carville K, Keaton J, Prentice J, Santamaria N (2009) Leg ulcers: atypical presentations and associated comorbidities. Wound Prac Res 17(4): 168–85
Reich-Schupke S, Doerler M, Wollina U, et al (2015) Squamous cell carcinoma in chronic venous leg ulcers. Data of the German Marjolin Registry and review. J Ditsch Dermatol Ges 13(10): 1006–13
Roewert-Huber J, Lange-Asschenfeldt B, Stockfleth E, Kerl H (2007) Epidemiology and aetiology of basal cell carcinoma. Br J Dermatol 157 Suppl 2: 47–51
Royal College of Nursing (2000) The Management of Patients With Venous Leg Ulcers. RCN, London. Available online: www.rcn.org.uk/professional-development/publications/pub-001269 (accessed January 2019)
Santilli MD, Santilli SM (1999) Chronic critical limb ischaemia: Diagnosis, treatment and prognosis. Am Fam Physician 59(7): 1899–1908. Available online: www.aafp.org/afp/1999/0401/p1899.html (accessed 10 January, 2019)
Telfer NR, Colver GB, Morton CA (2008) Guidelines for the management of basal cell carcinoma. Br J Dermatol 159: 35–48
Tobón J, Whitney JD, Jarrett M (2008) Nutritional status and wound severity of overweight and obese patients with venous leg ulcers: a pilot study. J Vasc Nurs 26(2): 43–52
Tokoro S, Satoh T, Okubo Y, Igawa K and Yokozeki H (2009) Latent dystrophic subcutaneous calcification in patients with chronic venous insufficiency. Acta Derma Venereol 89: 505–8
Wounds UK (2016) Best Practice Statement: Holistic management of venous leg ulceration. Wounds UK, London