

It is well established that lower limb complications in diabetes are the result of peripheral arterial disease (PAD; reduced blood flow to the limbs), neuropathy (loss of sensation), infection, or any combination of the three (Jeffcoate and Harding, 2003; Hinchcliffe et al, 2019; Lipsky et al, 2019). The sequence of foot ulceration tends to occur with underlying neuropathy and/or PAD as a precursor, followed by trauma that leads to tissue breakdown/ulceration (Jeffcoate and Harding, 2003; Clayton and Elsay, 2009). The ulcerative foot in diabetes can then deteriorate further due to PAD/ischaemia and/or infection, which leads to amputation. Infection of foot ulceration in diabetes increases amputation risk by 150 times compared to non-infected ulcers (Prompers et al, 2007; Figure 1).
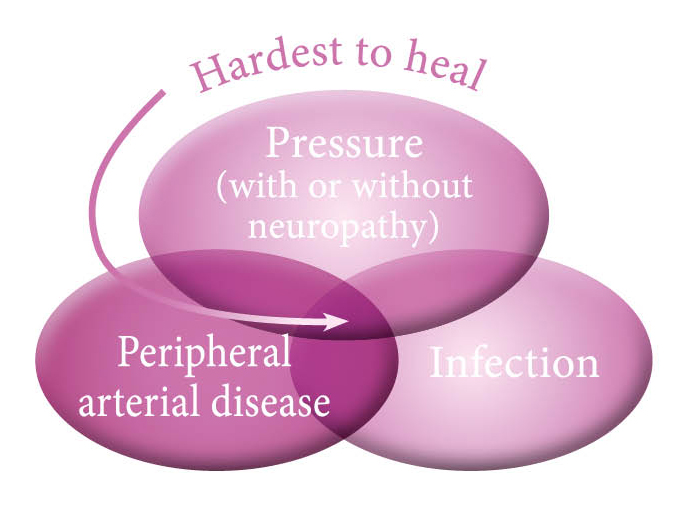
Figure 1. Hard-to-heal diabetic foot ulcer.
Infection
Infection is a continuum that can progress rapidly in the diabetic foot from a suspected colonised wound/ulcer to severe infection (Figure 2). It is the clinician’s responsibility to recognise covert signs (as listed below) of infection that may occur before the overt signs of infection characterised in Table 1. Prior to the presence of overt infection, there is believed to be a tipping point from wound contamination and colonisation leading to local infection. This perceived tipping point was historically called ‘critical colonisation’. However, this term is no longer advocated due to the lack of clarity in its definition and is now referred to as covert infection (International Wound Infection Institute [IWII], 2016).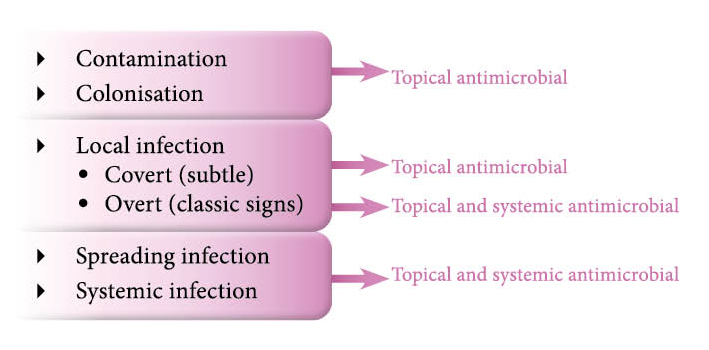
Figure 2. Continuum of infection.
Infection in the diabetic foot is not fully understood and is potentially over diagnosed and/or treated. Guest et al (2018) recognised that 14% of DFUs were documented as infected at initial presentation, with a further 31% documented as being treated with an antimicrobial. Therefore, up to 45% of DFUs may be infected at initial presentation. This is less than previously reported by Prompers et al (2007), who estimated the number of infected DFUs at initial presentation to be 58%, but similar to the figures reported by NDFA, which showed 43.6% of ulcers at presentation to MDFS having clinical signs of infection
(NDFA, 2019).
Where people are admitted to hospital because of DFUs, the number of people with infection increases to 82% (Prompers et al, 2007). Therefore, at initial presentation, the number of DFUs with infection is between 14% and 58%, rising to 82% if the first presentation is via admission. This is a significant spread and possibly implies the difficulty in diagnosing effectively, or else the overuse of antimicrobial agents in the treatment of DFUs.
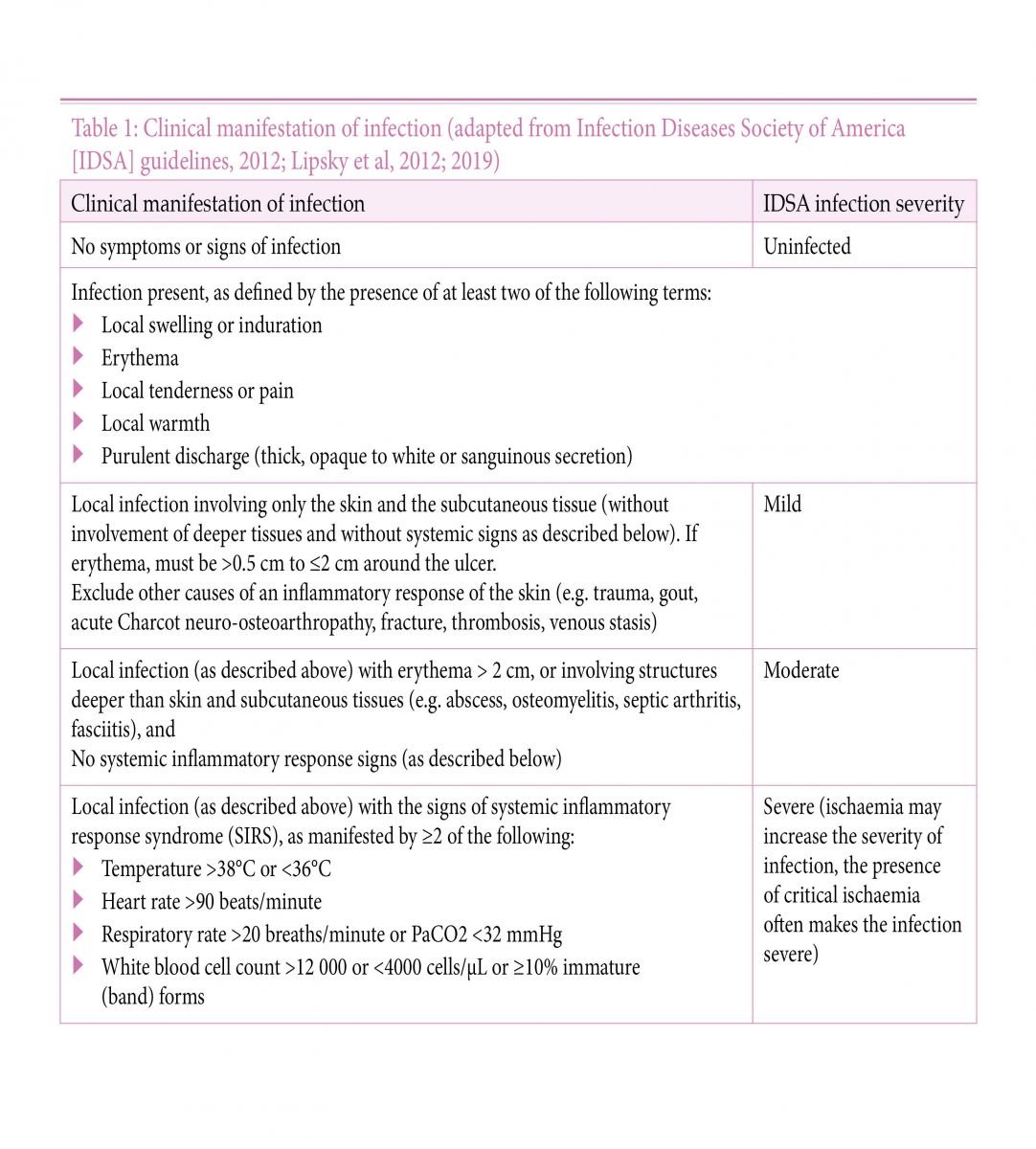

Figure 3. Charcot neuro-osteoarthropathy.
This 64-year-old male patient, with type 2 diabetes (20-year history), a body mass index (BMI) of 20, and known peripheral neuropathy presented to an outpatient clinic with a red, swollen, painful foot (Figure 4). His current medications were vitamin B compound, trazodone 50mg, thiamine 200mg, spironolactone 100mg, omeprazole 80mg, nirtazapine 45mg, metformin 1.5g, and folic acid 5mg.


He regularly attended ongoing treatment for active foot ulceration to the left foot and a recently healed ulcer to the right foot, with underlying osteomyelitis. On a particular occasion, he attended his weekly clinical review and mentioned that he had injured his right foot during the week. He recalled kicking a radiator, which caused a traumatic injury to his right foot. There was a 1x1.5cm (length x width) active ulcer to the dorsum of his right foot with redness, heat and swelling extending from the ulceration in the foot. At initial presentation, there was evidence of suspected clinical infection. The patient was suspected of having Charcot neuro-osteoarthropathy (Charcot foot) and possible undiagnosed underlying osteomyelitis. He was referred for X-ray and was currently on clindamycin 1.8g (450mg QDS) and ciprofloxacin 1g (500mg BD) for osteomyelitis in his right third and fifth toes.
Figure 4. Foot at initial presentation. Photographs reproduced
courtesy of Salford Royal NHS Foundation Trust.
courtesy of Salford Royal NHS Foundation Trust.
He regularly attended ongoing treatment for active foot ulceration to the left foot and a recently healed ulcer to the right foot, with underlying osteomyelitis. On a particular occasion, he attended his weekly clinical review and mentioned that he had injured his right foot during the week. He recalled kicking a radiator, which caused a traumatic injury to his right foot. There was a 1x1.5cm (length x width) active ulcer to the dorsum of his right foot with redness, heat and swelling extending from the ulceration in the foot. At initial presentation, there was evidence of suspected clinical infection. The patient was suspected of having Charcot neuro-osteoarthropathy (Charcot foot) and possible undiagnosed underlying osteomyelitis. He was referred for X-ray and was currently on clindamycin 1.8g (450mg QDS) and ciprofloxacin 1g (500mg BD) for osteomyelitis in his right third and fifth toes.
At initial X-ray there was no bony destruction noted (radiology reported that bones were osteopenic, no osteolysis or bony destruction to suggest frank osteomyelitis) and the patient was given a removable walker device, i.e. knee-to-toe offloading that offers similar offloading to a total contact cast but could be removed at night.
The patient had a history of ABPI assessments which showed incompressible arteries due to calcification. Toe pressures were done following traumatic injury, with an absolute toe pressure of 35mmHg, indicative of severe PAD. It was therefore decided that total contact casting was contraindicated due to severe PAD, and that the removable walker would be continued (Figure 5). Six days later, the foot’s architecture had severely collapsed with multiple fractures and dislocations, and so Charcot foot was confirmed. Unfortunately, due to the severity of the destruction, the associated PAD and ongoing ulceration and infection risk, the decision to perform below-knee amputation was taken. Management of the patient was through the MDFS clinic.


Figure 5. Foot five days later. Photographs reproduced courtesy of
Salford Royal NHS Foundation Trust.
The patient had a history of ABPI assessments which showed incompressible arteries due to calcification. Toe pressures were done following traumatic injury, with an absolute toe pressure of 35mmHg, indicative of severe PAD. It was therefore decided that total contact casting was contraindicated due to severe PAD, and that the removable walker would be continued (Figure 5). Six days later, the foot’s architecture had severely collapsed with multiple fractures and dislocations, and so Charcot foot was confirmed. Unfortunately, due to the severity of the destruction, the associated PAD and ongoing ulceration and infection risk, the decision to perform below-knee amputation was taken. Management of the patient was through the MDFS clinic.
Figure 5. Foot five days later. Photographs reproduced courtesy of
Salford Royal NHS Foundation Trust.
References
Abouhamda A, Alturkstani M, Jan Y (2019) Lower sensitivity of ankle-brachial index measurements among people suffering with diabetes-associated vascular disorders: A systematic review. SAGE open medicine 7, 2050312119835038
Alavi A, Sibbald RG, Nabavizadeh R, Valaei F, Coutts P, Mayer D (2015) Audible handheld Doppler ultrasound determines reliable and inexpensive exclusion of significant peripheral arterial disease. Vascular 23(6): 622–9
British Lymphology Society (2018) Position Paper for Ankle Brachial Pressure Index (ABPI). Informing decision making prior to the application of compression therapy. Available online: www.thebls.com
Brownrigg JRW, Schaper NC, Hinchcliffe RJ (2015) Diagnosis and assessment of peripheral arterial disease in the diabetic foot. Diabetic Med 32(6): 738–47
Buerger L (1924) Circulatory disturbances of the extremities. WB Saunders, Philadelphia: 162–8
Charnogursky G, Lee H, Lopez N (2014) Diabetic neuropathy. In: Handbook of Clinical Neurology. Vol 120. Elsevier: 773–85
Clayton W, Elsay TA (2009) A review of the pathophysiology, classification, and treatment of foot ulcers in diabetic patients. Clin Diabetes 27(2): 52–8
Concannon MJ, Sharpe A (2012) The importance of screening for Charcot neuroarthropathy. Practice Nurs 23(8), published online 29 Sept 2013
Conte MS, Bradbury AW, Kolh P, White JV, Dick F, Fitridge R, et al (2019) Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg 69(6S): 3S–125S
Department of Health (2019) The 9th annual report from the Advisory Committee on Antimicrobial Prescribing, Resistance and Healthcare Associated Infection (APRHAI). APRHAI annual report, 2017 to 2018. Available online: www.gov.uk/government/publications/aprhai-annual-report-2017-to-2018 (accessed 19 January, 2020)
Dolan NC, Liu K, Criqui MH, Greenland P, Guralnik JM, Chan C, et al (2002) Peripheral artery disease, diabetes, and reduced lower extremity functioning. Diabetes Care 25(1): 113–20
Guest JF, Fuller GW, Vowden P (2018) Diabetic foot ulcer management in clinical practice in the UK: costs and outcomes. Int Wound J 15(1): 43–52
Hinchliffe RJ, Forsythe RO, Apelqvist J, Boyko EJ, Fitridge R, Pio Hong J, et al on behalf of the International Working Group on the Diabetic Foot (2019) IWGDF Guideline on diagnosis, prognosis and management of peripheral artery disease in patients with a foot ulcer and diabetes. Available online: www.iwgdfguidelines.org
Hingorani A, LaMuraglia GM, Henke P, Meissner MH, Loretz L, Zinszer KM, et al (2016) The management of diabetic foot: A clinical practice guideline by the Society for Vascular Surgery in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine. J Vasc Surg 63(2 Suppl): 3S–21S
International Wound Infection Institute (2016) Wound Infection in Clinical Practice. International Consensus. Wounds International, London. Available online: https://bit.ly/2iWLDAc (accessed 9 January, 2020)
Jeffcoate WJ, Harding KG (2003) Diabetic foot ulcers. Lancet 361(9368): 1545–51
Keast D, Swanson T, Carville K, Fletcher J, Schultz G, Black J (2014) Ten Top Tips... understanding and managing wound biofilm. Wounds Int 5(2): 20–4
Lend GC, Fowkes FGR (1992) The Edinburgh Claudication Questionnaire: An improved version of the WHO/Rose questionnaire for use in epidemiological surveys. J Clin Epidemiol 45(10): 1101–09
Lipsky BA, Berendt AR, Cornia PB, Pile JC, Peters EJG, Armstrong DG, et al (2012) 2012 Infection Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Treatment of Diabetic Foot Infections. Clin Infect Dis 54(12): e132–2173
Lipsky BA, Senneville E, Abbas ZG, Aragón-Sánchez J, Diggle M, Embiln J, et al on behalf of the International Working Group on the Diabetic Foot (2019) IWGDF Guideline on the diagnosis and treatment of foot infection in persons with diabetes. Available online: www.iwgdfguidelines.org
Lundin M, Wiksten JP, Peräkylä T, Lindfors O, Savolainen H, Skyttä J, et al (1999) Distal pulse palpation: is it reliable? World J Surg 23(3): 252–5
McGee SR, Boyko EJ (1998) Physical examination and chronic lower-extremity ischemia: a critical review. Arch Intern Med 158(12): 1357–64
National Diabetes Footcare Audit (2019) National Diabetes Footcare Audit, 2014–2018. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/national-diabetes-footcare-audit/2014-2018. Accessed 19/01/2020
National Heart, Lung and Blood Institute (2019) Peripheral Arterial Disease. Available online: www.nhlbi.nih.gov/health-topics/peripheral-artery-disease (accessed 9 January, 2020)
National Institute for Health and Care Excellence (2018) Peripheral arterial disease: diagnosis and management. Clinical guideline [CG147]. NICE, London. Available online: www.nice.org.uk/guidance/cg147
National Institute for Health and Care Excellence (2019) Diabetic foot problems: prevention and management. NG19. NICE, London. Available online: www.nice.org.uk/guidance/ng19 (accessed 19 January, 2020)
Pham H, Armstrong DG, Harvey C, et al (2000) Screening techniques to identify people at high risk for diabetic foot ulceration: a prospective multicentre trial. Diabetes Care 23: 606–11
Prompers L, Huijberts M, Apelqvist J, Jude E, Piaggesi A, Bakker K, et al (2007) High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetlogia 50(1): 18–25
Rogers LC, Frykberg RG, Armstrong DG, Boulton AJM, Edmonds M, Ha Van G, et al (2011) The Charcot foot in diabetes. Diabetes Care 34(9): 2123–29
Scissons R (2008) Characterizing triphasic, biphasic, and monophasic Doppler waveforms: should a simple task be so difficult? J Diagnostic Med Sonography 24(5): 269–76
Society for Vascular Surgery Lower Extremity Guidelines Writing Group, Conte MS, Pomposelli FB, et al (2015) Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: management of asymptomatic disease and claudication. J Vasc Surg 61(3 suppl): 2S–41S
Teo KK (2019) Occlusive Peripheral Arterial Disease. MSD Manual. Available online: www.msdmanuals.com/en-gb/home/heart-and-blood-vessel-disorders/peripheral-arterial-disease/occlusive-peripheral-arterial-disease (accessed 9 January, 2020)
Alavi A, Sibbald RG, Nabavizadeh R, Valaei F, Coutts P, Mayer D (2015) Audible handheld Doppler ultrasound determines reliable and inexpensive exclusion of significant peripheral arterial disease. Vascular 23(6): 622–9
British Lymphology Society (2018) Position Paper for Ankle Brachial Pressure Index (ABPI). Informing decision making prior to the application of compression therapy. Available online: www.thebls.com
Brownrigg JRW, Schaper NC, Hinchcliffe RJ (2015) Diagnosis and assessment of peripheral arterial disease in the diabetic foot. Diabetic Med 32(6): 738–47
Buerger L (1924) Circulatory disturbances of the extremities. WB Saunders, Philadelphia: 162–8
Charnogursky G, Lee H, Lopez N (2014) Diabetic neuropathy. In: Handbook of Clinical Neurology. Vol 120. Elsevier: 773–85
Clayton W, Elsay TA (2009) A review of the pathophysiology, classification, and treatment of foot ulcers in diabetic patients. Clin Diabetes 27(2): 52–8
Concannon MJ, Sharpe A (2012) The importance of screening for Charcot neuroarthropathy. Practice Nurs 23(8), published online 29 Sept 2013
Conte MS, Bradbury AW, Kolh P, White JV, Dick F, Fitridge R, et al (2019) Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg 69(6S): 3S–125S
Department of Health (2019) The 9th annual report from the Advisory Committee on Antimicrobial Prescribing, Resistance and Healthcare Associated Infection (APRHAI). APRHAI annual report, 2017 to 2018. Available online: www.gov.uk/government/publications/aprhai-annual-report-2017-to-2018 (accessed 19 January, 2020)
Dolan NC, Liu K, Criqui MH, Greenland P, Guralnik JM, Chan C, et al (2002) Peripheral artery disease, diabetes, and reduced lower extremity functioning. Diabetes Care 25(1): 113–20
Guest JF, Fuller GW, Vowden P (2018) Diabetic foot ulcer management in clinical practice in the UK: costs and outcomes. Int Wound J 15(1): 43–52
Hinchliffe RJ, Forsythe RO, Apelqvist J, Boyko EJ, Fitridge R, Pio Hong J, et al on behalf of the International Working Group on the Diabetic Foot (2019) IWGDF Guideline on diagnosis, prognosis and management of peripheral artery disease in patients with a foot ulcer and diabetes. Available online: www.iwgdfguidelines.org
Hingorani A, LaMuraglia GM, Henke P, Meissner MH, Loretz L, Zinszer KM, et al (2016) The management of diabetic foot: A clinical practice guideline by the Society for Vascular Surgery in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine. J Vasc Surg 63(2 Suppl): 3S–21S
International Wound Infection Institute (2016) Wound Infection in Clinical Practice. International Consensus. Wounds International, London. Available online: https://bit.ly/2iWLDAc (accessed 9 January, 2020)
Jeffcoate WJ, Harding KG (2003) Diabetic foot ulcers. Lancet 361(9368): 1545–51
Keast D, Swanson T, Carville K, Fletcher J, Schultz G, Black J (2014) Ten Top Tips... understanding and managing wound biofilm. Wounds Int 5(2): 20–4
Lend GC, Fowkes FGR (1992) The Edinburgh Claudication Questionnaire: An improved version of the WHO/Rose questionnaire for use in epidemiological surveys. J Clin Epidemiol 45(10): 1101–09
Lipsky BA, Berendt AR, Cornia PB, Pile JC, Peters EJG, Armstrong DG, et al (2012) 2012 Infection Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Treatment of Diabetic Foot Infections. Clin Infect Dis 54(12): e132–2173
Lipsky BA, Senneville E, Abbas ZG, Aragón-Sánchez J, Diggle M, Embiln J, et al on behalf of the International Working Group on the Diabetic Foot (2019) IWGDF Guideline on the diagnosis and treatment of foot infection in persons with diabetes. Available online: www.iwgdfguidelines.org
Lundin M, Wiksten JP, Peräkylä T, Lindfors O, Savolainen H, Skyttä J, et al (1999) Distal pulse palpation: is it reliable? World J Surg 23(3): 252–5
McGee SR, Boyko EJ (1998) Physical examination and chronic lower-extremity ischemia: a critical review. Arch Intern Med 158(12): 1357–64
National Diabetes Footcare Audit (2019) National Diabetes Footcare Audit, 2014–2018. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/national-diabetes-footcare-audit/2014-2018. Accessed 19/01/2020
National Heart, Lung and Blood Institute (2019) Peripheral Arterial Disease. Available online: www.nhlbi.nih.gov/health-topics/peripheral-artery-disease (accessed 9 January, 2020)
National Institute for Health and Care Excellence (2018) Peripheral arterial disease: diagnosis and management. Clinical guideline [CG147]. NICE, London. Available online: www.nice.org.uk/guidance/cg147
National Institute for Health and Care Excellence (2019) Diabetic foot problems: prevention and management. NG19. NICE, London. Available online: www.nice.org.uk/guidance/ng19 (accessed 19 January, 2020)
Pham H, Armstrong DG, Harvey C, et al (2000) Screening techniques to identify people at high risk for diabetic foot ulceration: a prospective multicentre trial. Diabetes Care 23: 606–11
Prompers L, Huijberts M, Apelqvist J, Jude E, Piaggesi A, Bakker K, et al (2007) High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetlogia 50(1): 18–25
Rogers LC, Frykberg RG, Armstrong DG, Boulton AJM, Edmonds M, Ha Van G, et al (2011) The Charcot foot in diabetes. Diabetes Care 34(9): 2123–29
Scissons R (2008) Characterizing triphasic, biphasic, and monophasic Doppler waveforms: should a simple task be so difficult? J Diagnostic Med Sonography 24(5): 269–76
Society for Vascular Surgery Lower Extremity Guidelines Writing Group, Conte MS, Pomposelli FB, et al (2015) Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: management of asymptomatic disease and claudication. J Vasc Surg 61(3 suppl): 2S–41S
Teo KK (2019) Occlusive Peripheral Arterial Disease. MSD Manual. Available online: www.msdmanuals.com/en-gb/home/heart-and-blood-vessel-disorders/peripheral-arterial-disease/occlusive-peripheral-arterial-disease (accessed 9 January, 2020)