

 Figure 1. A malignant cavity wound.
Figure 1. A malignant cavity wound.
 Figure 2. A dehisced surgical cavity wound.
Figure 2. A dehisced surgical cavity wound.
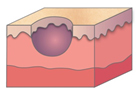
Figure 3a. A regular-shaped cavity, with uniform shape and sloping sides
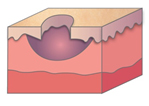
Figure 3b. A cavity with undermining (tissue destruction underneath intact skin around the wound margins
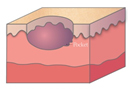
Figure 3c. A cavity with a tunnel (a pathway extending from the cavity) or pocket (an area of dead space)
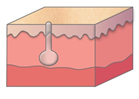
Figure 3d. A sinus (a blind-ended tunnel leading to a cavity which commonly contains a collection of infected matter)
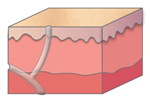
Figure 3e. A fistula (an abnormal tunnel connecting two organs or an organ to the skin)
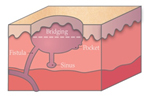
Figure 3f. A cavity wound with bridging (tissue that bridges one side on the cavity to another)

Figure 4. Reproduced with permission from Clare Morris, Tissue Viability Nurse Specialist

Figure 5. Maceration.

Figure 6. Day 1.

Figure 7. Day 4.

Figure 8. Day 10.

Figure 9. Day 23.

Figure 10. Day 63.

Figure 11. Day 74.

Figure 12. Day 103.
References
Brown A (2018) Diagnosing and managing infection in acute and chronic wounds. Nursing Times (online) 114(7): 36–41
Chadwick P, McCardle J (2016) Open, non-comparative, multicentre post clinical study of the performance and safety of a gelling fibre wound dressing on diabetic foot ulcers. J Wound Care 25(5): 290–300
Chaloner D, Poole M (1995) Cavity wound management in the community. Br J Nurs 4(10): 556–61
Charlesworth B, Pilling C, Chadwick P, Butcher M (2014) Dressing-related trauma: clinical sequelae and resource utilization in a UK setting. Clinicoeconomics and Outcomes Research 6: 227–39
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4010615/
Cooper P (2006) How to probe a wound during assessment to help determine treatment options. Wound Essentials (1): 87–9
European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance (2019) Prevention and treatment of pressure ulcers/injuries: Quick reference guide. Emily Haesler (Ed.). EPUAP/NPIAP/PPPIA, 2019
EWMA (2007) Position document: Topical negative pressure in wound management. MEP Ltd, London. Available online: www.ewma.org
Jones J (2006) The use of gauze: will it ever change? Int Wound J 3(2): 79–88
Guest JF, Ayoub N, Mcllwraith T et al (2015) Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5(12): e009283
Lindholm C, Bergsten A, Berglund E (1999) Chronic wounds and nursing care. J Wound Care 8(1): 5–10
Maddineni NK, Kodura SK, Surath S et al (2015) Negative pressure wound therapy in orthopaedic post-operative infections. Journal of NTR University Health Sciences 4(4): 257–62
Mahoney K (2020) Part 1: Wound assessment. J Comm Nurs 34(2): 28–35
Metcalf DG, Bowler PG, Hurlow J (2014) A clinical algorithm for wound biofilm identification. J Wound Care 23(3): 137–42
Morgan-Jones R, Bishay M, Hernández-Hermosa, JA, et al (2019) Consensus meeting report. Incision care and dressing selection in surgical wounds: Findings from an international meeting of surgeons. Wounds International, London. Available online: www.woundsinternational.com
Ousey K, O’Connor L, Doughty D, et al (2017) IAD Made Easy. Wound Int: 1–6
Phillips CJ, Humphreys I, Fletcher J et al (2015) Estimating the costs associated with the management of patients with chronic wounds using linked routine data. Int Wound J doi:10.1111/iwj.12443
Quain AM and Khardori NM (2015) Nutrition in Wound care Management: A Comprehensive overview. Wounds 27(12): 327–35
Skerritt L and Moore Z (2014) The prevalence, aetiology and management of wounds in a community care area in Ireland. Community Wound Care 19 (Sup6): S11–S17
Smet S (2015) An open, non-comparative, multicentre clinical investigation to evaluate the performance and safety of a gelling fibre dressing for the treatment of pressure ulcers. Poster presentation. European Pressure Ulcer Advisory Panel Conference. Gent, Belgium
Smith N, Overland J, Greenwood J (2015) Local management of deep cavity wounds – current and emerging therapies. Chronic Wound Care Management and Research (2): 159–70
Srinivasaiah N, Dugdall H, Barrett S et al (2007) A point prevalence survey of wounds in North east England. J Wound Care 16(10): 413–19
Timmons J, Cooper P (2008) How to systemically assess a patient with a cavity wound. Wounds UK Supplement (4)2: 4–10
Timmons J, Dugid K, Pirie G et al (2008) The management of a patient with a cavity wound. Wounds UK Supplement (4)2: 11–18
Vowden K (2016) Defining, assessing and managing cavity wounds. Wounds UK 12(1): 18–23
Vowden K, Vowden P (2014) Wound dressings: principles and practice, Surgery (Oxford) 35(9): 489–94
Williams C (1997) Treatment of cavity wounds. Practice Nursing 8(13): 31–33
White R (2005) Evidence for atraumatic soft silicone wound dressing use. Wounds UK 1(3): 104–9
White R (2008) A multinational survey of the assessment of pain when removing dressings. Wounds UK 4(1): 14–22
Wounds UK (2016) Quick Guide Cavity Wounds. Wounds UK, London. Available online: www.wounds-uk.com
Wounds UK (2018) Best practice statement: Improving holistic assessment of chronic wounds. Wounds UK, London. Available online: www.wounds-uk.com
WUWHS (2018) Consensus document. Surgical wound dehiscence: improving prevention and outcomes. Wounds International, London. Available online: www.woundsinternational.com
WUWHS (2019a) Consensus document. Wound exudate: effective assessment and management. Wounds International, London. Available online: www.woundsinternational.com
WUWHS (2019b) Consensus document. Surgical wound dehiscence: Improving prevention and outcomes. Wounds International, London. Available online: www.woundsinternational.com
Young T (2017) Back to basics: understanding moisture-associated skin damage. Wounds UK 13(2): 56–65
Chadwick P, McCardle J (2016) Open, non-comparative, multicentre post clinical study of the performance and safety of a gelling fibre wound dressing on diabetic foot ulcers. J Wound Care 25(5): 290–300
Chaloner D, Poole M (1995) Cavity wound management in the community. Br J Nurs 4(10): 556–61
Charlesworth B, Pilling C, Chadwick P, Butcher M (2014) Dressing-related trauma: clinical sequelae and resource utilization in a UK setting. Clinicoeconomics and Outcomes Research 6: 227–39
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4010615/
Cooper P (2006) How to probe a wound during assessment to help determine treatment options. Wound Essentials (1): 87–9
European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance (2019) Prevention and treatment of pressure ulcers/injuries: Quick reference guide. Emily Haesler (Ed.). EPUAP/NPIAP/PPPIA, 2019
EWMA (2007) Position document: Topical negative pressure in wound management. MEP Ltd, London. Available online: www.ewma.org
Jones J (2006) The use of gauze: will it ever change? Int Wound J 3(2): 79–88
Guest JF, Ayoub N, Mcllwraith T et al (2015) Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5(12): e009283
Lindholm C, Bergsten A, Berglund E (1999) Chronic wounds and nursing care. J Wound Care 8(1): 5–10
Maddineni NK, Kodura SK, Surath S et al (2015) Negative pressure wound therapy in orthopaedic post-operative infections. Journal of NTR University Health Sciences 4(4): 257–62
Mahoney K (2020) Part 1: Wound assessment. J Comm Nurs 34(2): 28–35
Metcalf DG, Bowler PG, Hurlow J (2014) A clinical algorithm for wound biofilm identification. J Wound Care 23(3): 137–42
Morgan-Jones R, Bishay M, Hernández-Hermosa, JA, et al (2019) Consensus meeting report. Incision care and dressing selection in surgical wounds: Findings from an international meeting of surgeons. Wounds International, London. Available online: www.woundsinternational.com
Ousey K, O’Connor L, Doughty D, et al (2017) IAD Made Easy. Wound Int: 1–6
Phillips CJ, Humphreys I, Fletcher J et al (2015) Estimating the costs associated with the management of patients with chronic wounds using linked routine data. Int Wound J doi:10.1111/iwj.12443
Quain AM and Khardori NM (2015) Nutrition in Wound care Management: A Comprehensive overview. Wounds 27(12): 327–35
Skerritt L and Moore Z (2014) The prevalence, aetiology and management of wounds in a community care area in Ireland. Community Wound Care 19 (Sup6): S11–S17
Smet S (2015) An open, non-comparative, multicentre clinical investigation to evaluate the performance and safety of a gelling fibre dressing for the treatment of pressure ulcers. Poster presentation. European Pressure Ulcer Advisory Panel Conference. Gent, Belgium
Smith N, Overland J, Greenwood J (2015) Local management of deep cavity wounds – current and emerging therapies. Chronic Wound Care Management and Research (2): 159–70
Srinivasaiah N, Dugdall H, Barrett S et al (2007) A point prevalence survey of wounds in North east England. J Wound Care 16(10): 413–19
Timmons J, Cooper P (2008) How to systemically assess a patient with a cavity wound. Wounds UK Supplement (4)2: 4–10
Timmons J, Dugid K, Pirie G et al (2008) The management of a patient with a cavity wound. Wounds UK Supplement (4)2: 11–18
Vowden K (2016) Defining, assessing and managing cavity wounds. Wounds UK 12(1): 18–23
Vowden K, Vowden P (2014) Wound dressings: principles and practice, Surgery (Oxford) 35(9): 489–94
Williams C (1997) Treatment of cavity wounds. Practice Nursing 8(13): 31–33
White R (2005) Evidence for atraumatic soft silicone wound dressing use. Wounds UK 1(3): 104–9
White R (2008) A multinational survey of the assessment of pain when removing dressings. Wounds UK 4(1): 14–22
Wounds UK (2016) Quick Guide Cavity Wounds. Wounds UK, London. Available online: www.wounds-uk.com
Wounds UK (2018) Best practice statement: Improving holistic assessment of chronic wounds. Wounds UK, London. Available online: www.wounds-uk.com
WUWHS (2018) Consensus document. Surgical wound dehiscence: improving prevention and outcomes. Wounds International, London. Available online: www.woundsinternational.com
WUWHS (2019a) Consensus document. Wound exudate: effective assessment and management. Wounds International, London. Available online: www.woundsinternational.com
WUWHS (2019b) Consensus document. Surgical wound dehiscence: Improving prevention and outcomes. Wounds International, London. Available online: www.woundsinternational.com
Young T (2017) Back to basics: understanding moisture-associated skin damage. Wounds UK 13(2): 56–65